{"title":"强直性脊柱炎的Andersson病变。","authors":"Xin Wu, Hongjuan Lu, Huji Xu","doi":"10.2478/rir-2022-0007","DOIUrl":null,"url":null,"abstract":"Road, Shanghai 200003, China. E-mail::xuhuji@smmu.edu.cn A 50-year-old male was admitted to our hospital due to “ recurrent back pain for 18 years, aggravated with numbness and weakness of the right lower limb for 3 months.” After admission, his physical examination showed that his spine activity was significantly limited. His HLA-B27 test was positive, and X-ray showed that his bilateral sacroiliac joint space had disappeared, hip joints were narrowed and femoral head was necrotized (Figure 1). Bone destruction was observed on the lower edge of T10 vertebral body and the upper edge of T11 vertebral body. Subsequent biopsy result revealed that the damage was not caused by tumor or infection. The patient was diagnosed as Ankylosing Spondylitis (AS) with Andersson lesion (AL). AL is a rare complication of AS, first described by Andersson in 1937.[1, 2] AL is a lesion of the intervertebral disk–vertebral interface at the late stage of AS, which can be characterized as a combination of bone hyperplasia and bone destruction. AL can be easily misdiagnosed as an infectious disease (such as spinal tuberculosis) or a neoplastic disease in clinical practice. The patient adopted surgical treatment and underwent standardized tumor necrosis factor antagonist (Etanercept) treatment after operation. So far, the patient’s pain and numbness of right lower limbs have significantly reduced. Conflict of Interest","PeriodicalId":74736,"journal":{"name":"Rheumatology and immunology research","volume":"3 1","pages":"45"},"PeriodicalIF":2.5000,"publicationDate":"2022-04-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e0/73/rir-03-045.PMC9524807.pdf","citationCount":"0","resultStr":"{\"title\":\"Andersson Lesion in Ankylosing Spondylitis.\",\"authors\":\"Xin Wu, Hongjuan Lu, Huji Xu\",\"doi\":\"10.2478/rir-2022-0007\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Road, Shanghai 200003, China. E-mail::xuhuji@smmu.edu.cn A 50-year-old male was admitted to our hospital due to “ recurrent back pain for 18 years, aggravated with numbness and weakness of the right lower limb for 3 months.” After admission, his physical examination showed that his spine activity was significantly limited. His HLA-B27 test was positive, and X-ray showed that his bilateral sacroiliac joint space had disappeared, hip joints were narrowed and femoral head was necrotized (Figure 1). Bone destruction was observed on the lower edge of T10 vertebral body and the upper edge of T11 vertebral body. Subsequent biopsy result revealed that the damage was not caused by tumor or infection. The patient was diagnosed as Ankylosing Spondylitis (AS) with Andersson lesion (AL). AL is a rare complication of AS, first described by Andersson in 1937.[1, 2] AL is a lesion of the intervertebral disk–vertebral interface at the late stage of AS, which can be characterized as a combination of bone hyperplasia and bone destruction. AL can be easily misdiagnosed as an infectious disease (such as spinal tuberculosis) or a neoplastic disease in clinical practice. The patient adopted surgical treatment and underwent standardized tumor necrosis factor antagonist (Etanercept) treatment after operation. So far, the patient’s pain and numbness of right lower limbs have significantly reduced. Conflict of Interest\",\"PeriodicalId\":74736,\"journal\":{\"name\":\"Rheumatology and immunology research\",\"volume\":\"3 1\",\"pages\":\"45\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2022-04-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e0/73/rir-03-045.PMC9524807.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Rheumatology and immunology research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2478/rir-2022-0007\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/3/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Rheumatology and immunology research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2478/rir-2022-0007","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/3/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
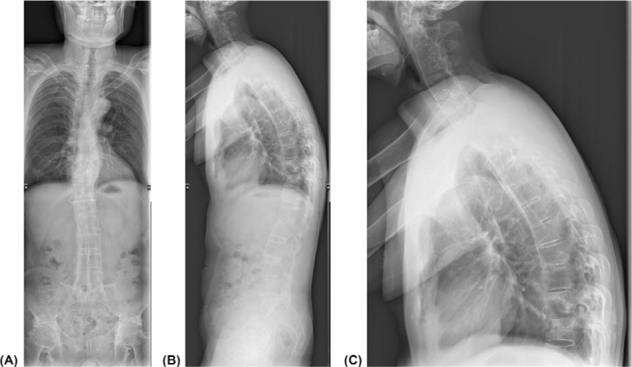
Road, Shanghai 200003, China. E-mail::xuhuji@smmu.edu.cn A 50-year-old male was admitted to our hospital due to “ recurrent back pain for 18 years, aggravated with numbness and weakness of the right lower limb for 3 months.” After admission, his physical examination showed that his spine activity was significantly limited. His HLA-B27 test was positive, and X-ray showed that his bilateral sacroiliac joint space had disappeared, hip joints were narrowed and femoral head was necrotized (Figure 1). Bone destruction was observed on the lower edge of T10 vertebral body and the upper edge of T11 vertebral body. Subsequent biopsy result revealed that the damage was not caused by tumor or infection. The patient was diagnosed as Ankylosing Spondylitis (AS) with Andersson lesion (AL). AL is a rare complication of AS, first described by Andersson in 1937.[1, 2] AL is a lesion of the intervertebral disk–vertebral interface at the late stage of AS, which can be characterized as a combination of bone hyperplasia and bone destruction. AL can be easily misdiagnosed as an infectious disease (such as spinal tuberculosis) or a neoplastic disease in clinical practice. The patient adopted surgical treatment and underwent standardized tumor necrosis factor antagonist (Etanercept) treatment after operation. So far, the patient’s pain and numbness of right lower limbs have significantly reduced. Conflict of Interest


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
