{"title":"关于肾上腺素自动注射器剂量的国际建议往往不同于基于体重的标准指南:回顾与临床建议。","authors":"Sten Dreborg, Graham Walter, Harold Kim","doi":"10.1186/s13223-022-00736-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In anaphylaxis, the dosing of injectable epinephrine in medical settings has been arbitrarily recommended to be 0.01 mg/kg of body weight. For ethical reasons, there have been no dose-response studies or double-blind studies performed on patients with active anaphylaxis. Intramuscular delivery of epinephrine has been the standard. Auto-injectors for use in the treatment of anaphylaxis are available in four strengths (0.1, 0.15, 0.3, and 0.5 mg). However, in many countries, only the 0.15 and 0.3 mg strengths are available. Consequently, many adult, heavy patients are prescribed the 0.3 mg dose, which may result in only one-fifth to one-third of the recommended weight-based dose being administered in heavy patients experiencing anaphylaxis. Underdosing may have therefore contributed to mortality in anaphylaxis.</p><p><strong>Objective: </strong>To review the doses of epinephrine recommended for the treatment of anaphylaxis in the community, and assess whether recommendations should be made to increase dosing for heavy adult patients in hopes of avoiding future deaths from anaphylaxis.</p><p><strong>Methods: </strong>We reviewed multiple national and international recommendations for the dosing of epinephrine. We also reviewed the literature on adverse drug reactions from epinephrine, lethal doses of epinephrine, and epinephrine dose-finding studies.</p><p><strong>Results: </strong>The majority of national and regional professional societies and authorities recommend epinephrine delivered by auto-injectors at doses far lower than the generally accepted therapeutic dose of 0.01 mg/kg body weight. Furthermore, we found that the recommendations vary even within regions themselves.</p><p><strong>Conclusions: </strong>We suggest prescribing more appropriate doses of epinephrine auto-injectors based on weight-based recommendations. There may be some exceptions, such as for patients with heart disease. We hypothesize that these recommendations will lead to improved outcomes of anaphylaxis.</p>","PeriodicalId":7702,"journal":{"name":"Allergy, Asthma, and Clinical Immunology : Official Journal of the Canadian Society of Allergy and Clinical Immunology","volume":" ","pages":"102"},"PeriodicalIF":0.0000,"publicationDate":"2022-12-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9724388/pdf/","citationCount":"0","resultStr":"{\"title\":\"International recommendations on epinephrine auto-injector doses often differ from standard weight-based guidance: a review and clinical proposals.\",\"authors\":\"Sten Dreborg, Graham Walter, Harold Kim\",\"doi\":\"10.1186/s13223-022-00736-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>In anaphylaxis, the dosing of injectable epinephrine in medical settings has been arbitrarily recommended to be 0.01 mg/kg of body weight. For ethical reasons, there have been no dose-response studies or double-blind studies performed on patients with active anaphylaxis. Intramuscular delivery of epinephrine has been the standard. Auto-injectors for use in the treatment of anaphylaxis are available in four strengths (0.1, 0.15, 0.3, and 0.5 mg). However, in many countries, only the 0.15 and 0.3 mg strengths are available. Consequently, many adult, heavy patients are prescribed the 0.3 mg dose, which may result in only one-fifth to one-third of the recommended weight-based dose being administered in heavy patients experiencing anaphylaxis. Underdosing may have therefore contributed to mortality in anaphylaxis.</p><p><strong>Objective: </strong>To review the doses of epinephrine recommended for the treatment of anaphylaxis in the community, and assess whether recommendations should be made to increase dosing for heavy adult patients in hopes of avoiding future deaths from anaphylaxis.</p><p><strong>Methods: </strong>We reviewed multiple national and international recommendations for the dosing of epinephrine. We also reviewed the literature on adverse drug reactions from epinephrine, lethal doses of epinephrine, and epinephrine dose-finding studies.</p><p><strong>Results: </strong>The majority of national and regional professional societies and authorities recommend epinephrine delivered by auto-injectors at doses far lower than the generally accepted therapeutic dose of 0.01 mg/kg body weight. Furthermore, we found that the recommendations vary even within regions themselves.</p><p><strong>Conclusions: </strong>We suggest prescribing more appropriate doses of epinephrine auto-injectors based on weight-based recommendations. There may be some exceptions, such as for patients with heart disease. We hypothesize that these recommendations will lead to improved outcomes of anaphylaxis.</p>\",\"PeriodicalId\":7702,\"journal\":{\"name\":\"Allergy, Asthma, and Clinical Immunology : Official Journal of the Canadian Society of Allergy and Clinical Immunology\",\"volume\":\" \",\"pages\":\"102\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-12-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9724388/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Allergy, Asthma, and Clinical Immunology : Official Journal of the Canadian Society of Allergy and Clinical Immunology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13223-022-00736-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Allergy, Asthma, and Clinical Immunology : Official Journal of the Canadian Society of Allergy and Clinical Immunology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13223-022-00736-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
International recommendations on epinephrine auto-injector doses often differ from standard weight-based guidance: a review and clinical proposals.
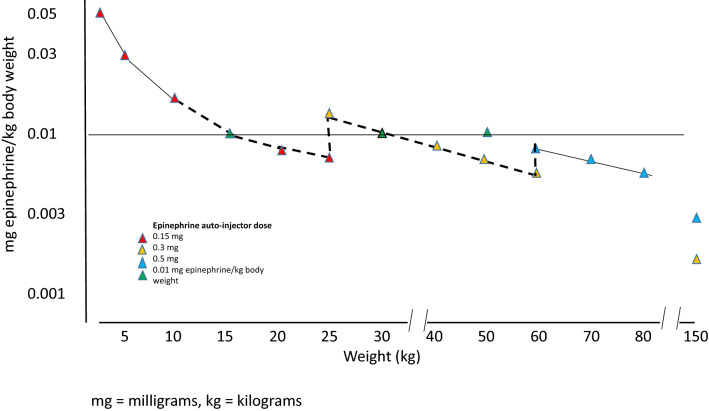
Background: In anaphylaxis, the dosing of injectable epinephrine in medical settings has been arbitrarily recommended to be 0.01 mg/kg of body weight. For ethical reasons, there have been no dose-response studies or double-blind studies performed on patients with active anaphylaxis. Intramuscular delivery of epinephrine has been the standard. Auto-injectors for use in the treatment of anaphylaxis are available in four strengths (0.1, 0.15, 0.3, and 0.5 mg). However, in many countries, only the 0.15 and 0.3 mg strengths are available. Consequently, many adult, heavy patients are prescribed the 0.3 mg dose, which may result in only one-fifth to one-third of the recommended weight-based dose being administered in heavy patients experiencing anaphylaxis. Underdosing may have therefore contributed to mortality in anaphylaxis.
Objective: To review the doses of epinephrine recommended for the treatment of anaphylaxis in the community, and assess whether recommendations should be made to increase dosing for heavy adult patients in hopes of avoiding future deaths from anaphylaxis.
Methods: We reviewed multiple national and international recommendations for the dosing of epinephrine. We also reviewed the literature on adverse drug reactions from epinephrine, lethal doses of epinephrine, and epinephrine dose-finding studies.
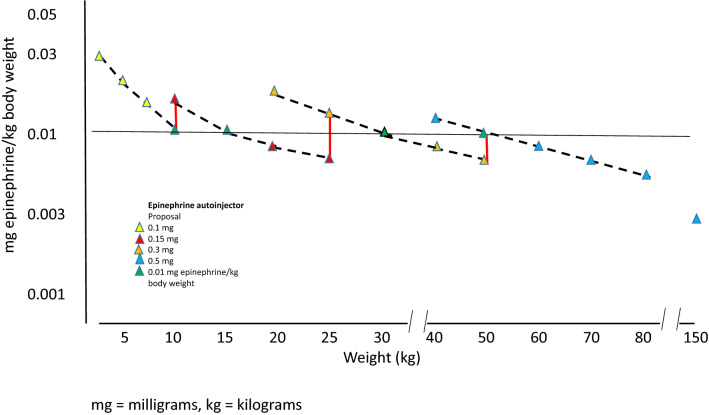
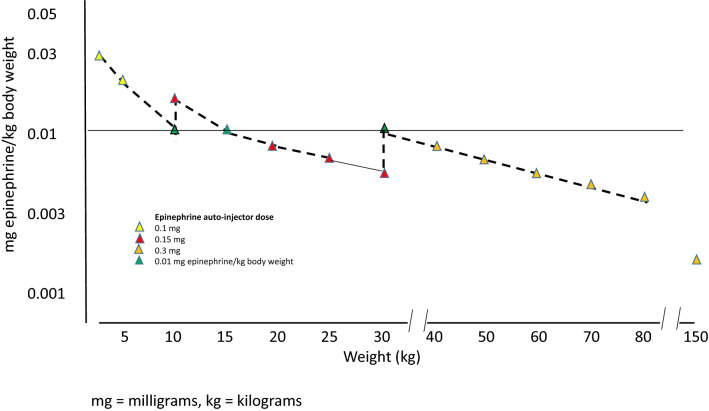
Results: The majority of national and regional professional societies and authorities recommend epinephrine delivered by auto-injectors at doses far lower than the generally accepted therapeutic dose of 0.01 mg/kg body weight. Furthermore, we found that the recommendations vary even within regions themselves.
Conclusions: We suggest prescribing more appropriate doses of epinephrine auto-injectors based on weight-based recommendations. There may be some exceptions, such as for patients with heart disease. We hypothesize that these recommendations will lead to improved outcomes of anaphylaxis.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
