{"title":"尿中性粒细胞明胶酶相关脂钙蛋白作为急性肾损伤、严重肾损伤和重症监护病房肾替代治疗需求的预测因子。","authors":"Fatma I Albeladi, Haifa M Algethamy","doi":"10.1159/000477469","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Recent attempts were made to identify early indicators of acute kidney injury (AKI) in order to accelerate treatment and hopefully improve outcomes. This study aims to assess the value of urinary neutrophil gelatinase-associated lipocalin (uNGAL) as a predictor of AKI, severe AKI, and the need for renal replacement therapy (RRT).</p><p><strong>Methods: </strong>We conducted a prospective study and included adults admitted to our intensive care unit (ICU) at King Abdulaziz University Hospital (KAUH), between May 2012 and June 2013, who had at least 1 major risk factor for AKI. They were followed up throughout their hospital stay to identify which potential characteristics predicted any of the above 3 outcomes. We collected information on patients' age and gender, the Acute Physiology And Chronic Health Evaluation, version II (APACHE II) score, the Sepsis-Related Organ Failure Assessment (SOFA) score, serum creatinine and cystatin C levels, and uNGAL. We compared ICU patients who presented with any of the 3 outcomes with others who did not.</p><p><strong>Results: </strong>We included 75 patients, and among those 21 developed AKI, 18 severe AKI, and 17 required RRT. Bivariate analysis revealed intergroup differences for almost all clinical variables (e.g., patients with AKI vs. patients without AKI); while multivariate analysis identified mean arterial pressure as the only predictor for AKI (<i>p</i> < 0.001) and the SOFA score (<i>p</i> = 0.04) as the only predictor for severe AKI. For RRT, day 1 maximum uNGAL was the stronger predictor (<i>p</i> < 0.001) when compared to admission diagnosis (<i>p</i> = 0.014). Day 1 and day 2 maximum uNGAL levels were good and excellent predictors for future RRT, but only fair to good predictors for AKI and severe AKI.</p><p><strong>Conclusions: </strong>Maximum urine levels of uNGAL measured over the first and second 24 h of an ICU admission were highly accurate predictors of the future need for RRT, however less accurate at detecting early and severe AKI.</p>","PeriodicalId":56356,"journal":{"name":"Nephron Extra","volume":"7 2","pages":"62-77"},"PeriodicalIF":0.0000,"publicationDate":"2017-07-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1159/000477469","citationCount":"15","resultStr":"{\"title\":\"Urinary Neutrophil Gelatinase-Associated Lipocalin as a Predictor of Acute Kidney Injury, Severe Kidney Injury, and the Need for Renal Replacement Therapy in the Intensive Care Unit.\",\"authors\":\"Fatma I Albeladi, Haifa M Algethamy\",\"doi\":\"10.1159/000477469\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Recent attempts were made to identify early indicators of acute kidney injury (AKI) in order to accelerate treatment and hopefully improve outcomes. This study aims to assess the value of urinary neutrophil gelatinase-associated lipocalin (uNGAL) as a predictor of AKI, severe AKI, and the need for renal replacement therapy (RRT).</p><p><strong>Methods: </strong>We conducted a prospective study and included adults admitted to our intensive care unit (ICU) at King Abdulaziz University Hospital (KAUH), between May 2012 and June 2013, who had at least 1 major risk factor for AKI. They were followed up throughout their hospital stay to identify which potential characteristics predicted any of the above 3 outcomes. We collected information on patients' age and gender, the Acute Physiology And Chronic Health Evaluation, version II (APACHE II) score, the Sepsis-Related Organ Failure Assessment (SOFA) score, serum creatinine and cystatin C levels, and uNGAL. We compared ICU patients who presented with any of the 3 outcomes with others who did not.</p><p><strong>Results: </strong>We included 75 patients, and among those 21 developed AKI, 18 severe AKI, and 17 required RRT. Bivariate analysis revealed intergroup differences for almost all clinical variables (e.g., patients with AKI vs. patients without AKI); while multivariate analysis identified mean arterial pressure as the only predictor for AKI (<i>p</i> < 0.001) and the SOFA score (<i>p</i> = 0.04) as the only predictor for severe AKI. For RRT, day 1 maximum uNGAL was the stronger predictor (<i>p</i> < 0.001) when compared to admission diagnosis (<i>p</i> = 0.014). Day 1 and day 2 maximum uNGAL levels were good and excellent predictors for future RRT, but only fair to good predictors for AKI and severe AKI.</p><p><strong>Conclusions: </strong>Maximum urine levels of uNGAL measured over the first and second 24 h of an ICU admission were highly accurate predictors of the future need for RRT, however less accurate at detecting early and severe AKI.</p>\",\"PeriodicalId\":56356,\"journal\":{\"name\":\"Nephron Extra\",\"volume\":\"7 2\",\"pages\":\"62-77\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2017-07-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1159/000477469\",\"citationCount\":\"15\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nephron Extra\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000477469\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/5/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nephron Extra","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000477469","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/5/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Urinary Neutrophil Gelatinase-Associated Lipocalin as a Predictor of Acute Kidney Injury, Severe Kidney Injury, and the Need for Renal Replacement Therapy in the Intensive Care Unit.
Background: Recent attempts were made to identify early indicators of acute kidney injury (AKI) in order to accelerate treatment and hopefully improve outcomes. This study aims to assess the value of urinary neutrophil gelatinase-associated lipocalin (uNGAL) as a predictor of AKI, severe AKI, and the need for renal replacement therapy (RRT).
Methods: We conducted a prospective study and included adults admitted to our intensive care unit (ICU) at King Abdulaziz University Hospital (KAUH), between May 2012 and June 2013, who had at least 1 major risk factor for AKI. They were followed up throughout their hospital stay to identify which potential characteristics predicted any of the above 3 outcomes. We collected information on patients' age and gender, the Acute Physiology And Chronic Health Evaluation, version II (APACHE II) score, the Sepsis-Related Organ Failure Assessment (SOFA) score, serum creatinine and cystatin C levels, and uNGAL. We compared ICU patients who presented with any of the 3 outcomes with others who did not.
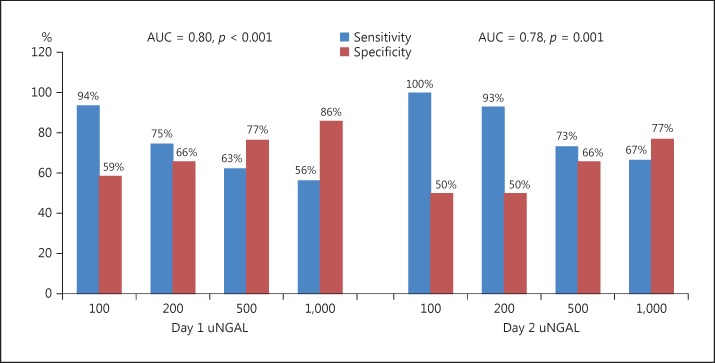
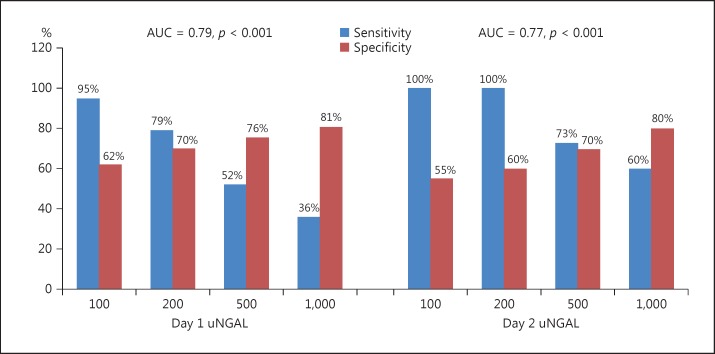
Results: We included 75 patients, and among those 21 developed AKI, 18 severe AKI, and 17 required RRT. Bivariate analysis revealed intergroup differences for almost all clinical variables (e.g., patients with AKI vs. patients without AKI); while multivariate analysis identified mean arterial pressure as the only predictor for AKI (p < 0.001) and the SOFA score (p = 0.04) as the only predictor for severe AKI. For RRT, day 1 maximum uNGAL was the stronger predictor (p < 0.001) when compared to admission diagnosis (p = 0.014). Day 1 and day 2 maximum uNGAL levels were good and excellent predictors for future RRT, but only fair to good predictors for AKI and severe AKI.
Conclusions: Maximum urine levels of uNGAL measured over the first and second 24 h of an ICU admission were highly accurate predictors of the future need for RRT, however less accurate at detecting early and severe AKI.
期刊介绍:
An open-access subjournal to Nephron. ''Nephron EXTRA'' publishes additional high-quality articles that cannot be published in the main journal ''Nephron'' due to space limitations.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
