Katherine Kolor, Zhuo Chen, Scott D Grosse, Juan L Rodriguez, Ridgely Fisk Green, W David Dotson, M Scott Bowen, Julie A Lynch, Muin J Khoury
{"title":"2009-2014年,美国非大都市和大都市地区18-64岁雇主赞助医疗保险的女性BRCA基因检测和预防性干预的接受情况。","authors":"Katherine Kolor, Zhuo Chen, Scott D Grosse, Juan L Rodriguez, Ridgely Fisk Green, W David Dotson, M Scott Bowen, Julie A Lynch, Muin J Khoury","doi":"10.15585/mmwr.ss6615a1","DOIUrl":null,"url":null,"abstract":"<p><strong>Problem/condition: </strong>Genetic testing for breast cancer 1 (BRCA1) and breast cancer 2 (BRCA2) gene mutations can identify women at increased risk for breast and ovarian cancer. These testing results can be used to select preventive interventions and guide treatment. Differences between nonmetropolitan and metropolitan populations in rates of BRCA testing and receipt of preventive interventions after testing have not previously been examined.</p><p><strong>Period covered: </strong>2009-2014.</p><p><strong>Description of system: </strong>Medical claims data from Truven Health Analytics MarketScan Commercial Claims and Encounters databases were used to estimate rates of BRCA testing and receipt of preventive interventions after BRCA testing among women aged 18-64 years with employer-sponsored health insurance in metropolitan and nonmetropolitan areas of the United States, both nationally and regionally.</p><p><strong>Results: </strong>From 2009 to 2014, BRCA testing rates per 100,000 women aged 18-64 years with employer-sponsored health insurance increased 2.3 times (102.7 to 237.8) in metropolitan areas and 3.0 times (64.8 to 191.3) in nonmetropolitan areas. The relative difference in BRCA testing rates between metropolitan and nonmetropolitan areas decreased from 37% in 2009 (102.7 versus 64.8) to 20% in 2014 (237.8 versus 191.3). The relative difference in BRCA testing rates between metropolitan and nonmetropolitan areas decreased more over time in younger women than in older women and decreased in all regions except the West. Receipt of preventive services 90 days after BRCA testing in metropolitan versus nonmetropolitan areas throughout the period varied by service: the percentage of women who received a mastectomy was similar, the percentage of women who received magnetic resonance imaging of the breast was lower in nonmetropolitan areas (as low as 5.8% in 2014 to as high as 8.2% in 2011) than metropolitan areas (as low as 7.3% in 2014 to as high as 10.3% in 2011), and the percentage of women who received mammography was lower in nonmetropolitan areas in earlier years but was similar in later years.</p><p><strong>Interpretation: </strong>Possible explanations for the 47% decrease in the relative difference in BRCA testing rates over the study period include increased access to genetic services in nonmetropolitan areas and increased demand nationally as a result of publicity. The relative differences in metropolitan and nonmetropolitan BRCA testing rates were smaller among women at younger ages compared with older ages.</p><p><strong>Public health action: </strong>Improved data sources and surveillance tools are needed to gather comprehensive data on BRCA testing in the United States, monitor adherence to evidence-based guidelines for BRCA testing, and assess receipt of preventive interventions for women with BRCA mutations. Programs can build on the recent decrease in geographic disparities in receipt of BRCA testing while simultaneously educating the public and health care providers about U.S. Preventive Services Task Force recommendations and other clinical guidelines for BRCA testing and counseling.</p>","PeriodicalId":48549,"journal":{"name":"Mmwr Surveillance Summaries","volume":"66 15","pages":"1-11"},"PeriodicalIF":49.8000,"publicationDate":"2017-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5879728/pdf/","citationCount":"59","resultStr":"{\"title\":\"BRCA Genetic Testing and Receipt of Preventive Interventions Among Women Aged 18-64 Years with Employer-Sponsored Health Insurance in Nonmetropolitan and Metropolitan Areas - United States, 2009-2014.\",\"authors\":\"Katherine Kolor, Zhuo Chen, Scott D Grosse, Juan L Rodriguez, Ridgely Fisk Green, W David Dotson, M Scott Bowen, Julie A Lynch, Muin J Khoury\",\"doi\":\"10.15585/mmwr.ss6615a1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Problem/condition: </strong>Genetic testing for breast cancer 1 (BRCA1) and breast cancer 2 (BRCA2) gene mutations can identify women at increased risk for breast and ovarian cancer. These testing results can be used to select preventive interventions and guide treatment. Differences between nonmetropolitan and metropolitan populations in rates of BRCA testing and receipt of preventive interventions after testing have not previously been examined.</p><p><strong>Period covered: </strong>2009-2014.</p><p><strong>Description of system: </strong>Medical claims data from Truven Health Analytics MarketScan Commercial Claims and Encounters databases were used to estimate rates of BRCA testing and receipt of preventive interventions after BRCA testing among women aged 18-64 years with employer-sponsored health insurance in metropolitan and nonmetropolitan areas of the United States, both nationally and regionally.</p><p><strong>Results: </strong>From 2009 to 2014, BRCA testing rates per 100,000 women aged 18-64 years with employer-sponsored health insurance increased 2.3 times (102.7 to 237.8) in metropolitan areas and 3.0 times (64.8 to 191.3) in nonmetropolitan areas. The relative difference in BRCA testing rates between metropolitan and nonmetropolitan areas decreased from 37% in 2009 (102.7 versus 64.8) to 20% in 2014 (237.8 versus 191.3). The relative difference in BRCA testing rates between metropolitan and nonmetropolitan areas decreased more over time in younger women than in older women and decreased in all regions except the West. Receipt of preventive services 90 days after BRCA testing in metropolitan versus nonmetropolitan areas throughout the period varied by service: the percentage of women who received a mastectomy was similar, the percentage of women who received magnetic resonance imaging of the breast was lower in nonmetropolitan areas (as low as 5.8% in 2014 to as high as 8.2% in 2011) than metropolitan areas (as low as 7.3% in 2014 to as high as 10.3% in 2011), and the percentage of women who received mammography was lower in nonmetropolitan areas in earlier years but was similar in later years.</p><p><strong>Interpretation: </strong>Possible explanations for the 47% decrease in the relative difference in BRCA testing rates over the study period include increased access to genetic services in nonmetropolitan areas and increased demand nationally as a result of publicity. The relative differences in metropolitan and nonmetropolitan BRCA testing rates were smaller among women at younger ages compared with older ages.</p><p><strong>Public health action: </strong>Improved data sources and surveillance tools are needed to gather comprehensive data on BRCA testing in the United States, monitor adherence to evidence-based guidelines for BRCA testing, and assess receipt of preventive interventions for women with BRCA mutations. Programs can build on the recent decrease in geographic disparities in receipt of BRCA testing while simultaneously educating the public and health care providers about U.S. Preventive Services Task Force recommendations and other clinical guidelines for BRCA testing and counseling.</p>\",\"PeriodicalId\":48549,\"journal\":{\"name\":\"Mmwr Surveillance Summaries\",\"volume\":\"66 15\",\"pages\":\"1-11\"},\"PeriodicalIF\":49.8000,\"publicationDate\":\"2017-09-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5879728/pdf/\",\"citationCount\":\"59\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Mmwr Surveillance Summaries\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.15585/mmwr.ss6615a1\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mmwr Surveillance Summaries","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.15585/mmwr.ss6615a1","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 59
摘要
问题/状况:乳腺癌1号(BRCA1)和乳腺癌2号(BRCA2)基因突变的基因检测可以识别出乳腺癌和卵巢癌风险增加的女性。这些检测结果可用于选择预防干预措施和指导治疗。非大都市人群和大都市人群在BRCA检测率和检测后接受预防性干预措施方面的差异此前未被研究过。涵盖期间:2009-2014年。系统描述:来自Truven Health Analytics MarketScan Commercial claims和Encounters数据库的医疗索赔数据被用于估计美国大都市和非大都市地区18-64岁雇主赞助的健康保险女性的BRCA检测率和BRCA检测后预防性干预的接受率,包括国家和地区。结果:2009 - 2014年,大城市地区每10万名18-64岁雇主赞助医疗保险女性的BRCA检测率增加了2.3倍(102.7至237.8),非大城市地区增加了3.0倍(64.8至191.3)。大都市和非大都市地区BRCA检测率的相对差异从2009年的37%(102.7对64.8)下降到2014年的20%(237.8对191.3)。随着时间的推移,年轻女性和非大都市地区BRCA检测率的相对差异比老年女性下降得更多,除西部地区外,所有地区都有所下降。在大都市地区和非大都市地区,BRCA检测后90天内接受预防服务的情况因服务而异:妇女接受乳房切除术的比例是相似的,女性的比例接受核磁共振成像的乳房nonmetropolitan地区较低(低至2014年的5.8%到2011年高达8.2%)比大城市(低至2014年的7.3%到2011年高达10.3%),和妇女接受乳房x光检查的百分比低nonmetropolitan地区早些年但在晚年很相似。解释:在研究期间,BRCA检测率的相对差异降低了47%,可能的解释包括非大都市地区获得遗传服务的机会增加,以及由于宣传而导致全国需求增加。与老年妇女相比,年轻妇女在大都市和非大都市BRCA检测率上的相对差异较小。公共卫生行动:需要改进数据来源和监测工具,以收集美国BRCA检测的综合数据,监测BRCA检测循证指南的遵守情况,并评估BRCA突变妇女预防性干预措施的接受情况。项目可以建立在最近接受BRCA检测的地域差异减少的基础上,同时教育公众和卫生保健提供者关于美国预防服务工作组的建议和其他BRCA检测和咨询的临床指南。
BRCA Genetic Testing and Receipt of Preventive Interventions Among Women Aged 18-64 Years with Employer-Sponsored Health Insurance in Nonmetropolitan and Metropolitan Areas - United States, 2009-2014.
Problem/condition: Genetic testing for breast cancer 1 (BRCA1) and breast cancer 2 (BRCA2) gene mutations can identify women at increased risk for breast and ovarian cancer. These testing results can be used to select preventive interventions and guide treatment. Differences between nonmetropolitan and metropolitan populations in rates of BRCA testing and receipt of preventive interventions after testing have not previously been examined.
Period covered: 2009-2014.
Description of system: Medical claims data from Truven Health Analytics MarketScan Commercial Claims and Encounters databases were used to estimate rates of BRCA testing and receipt of preventive interventions after BRCA testing among women aged 18-64 years with employer-sponsored health insurance in metropolitan and nonmetropolitan areas of the United States, both nationally and regionally.
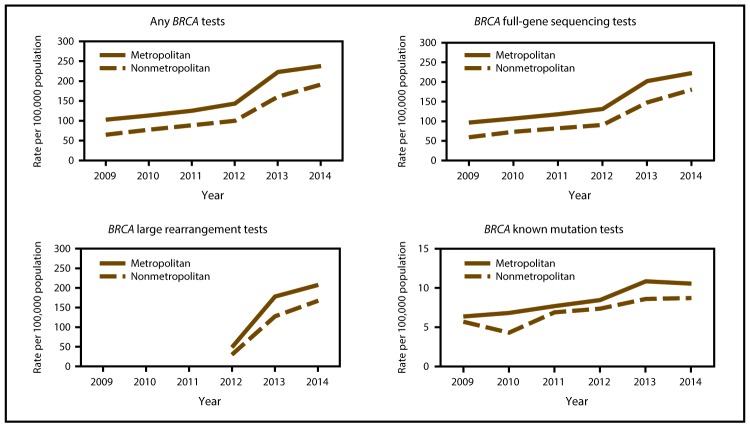
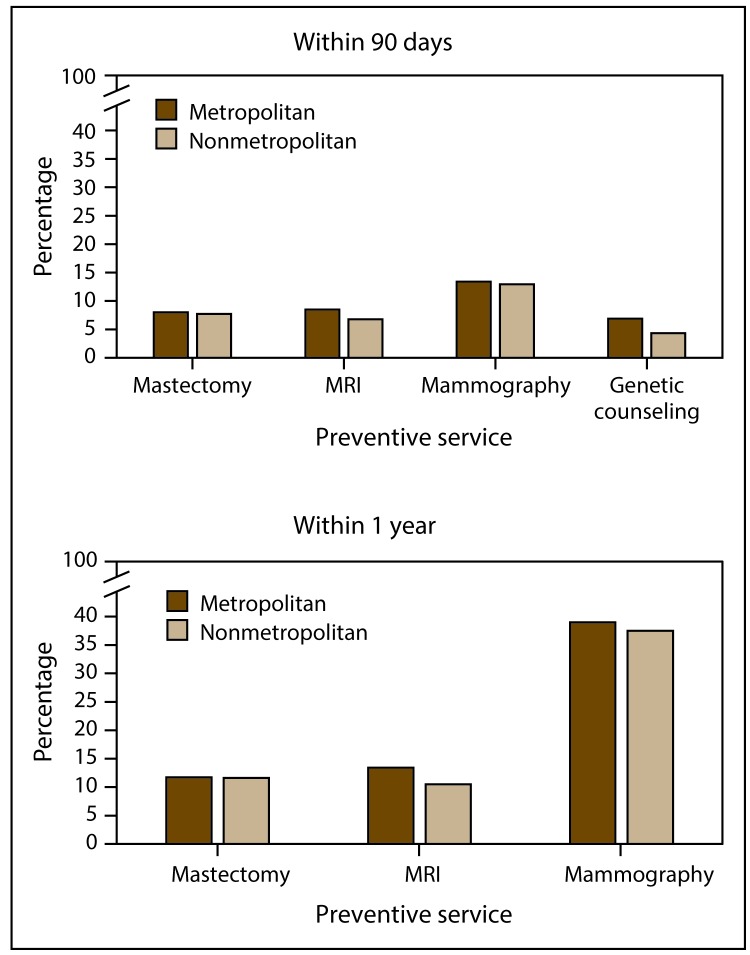
Results: From 2009 to 2014, BRCA testing rates per 100,000 women aged 18-64 years with employer-sponsored health insurance increased 2.3 times (102.7 to 237.8) in metropolitan areas and 3.0 times (64.8 to 191.3) in nonmetropolitan areas. The relative difference in BRCA testing rates between metropolitan and nonmetropolitan areas decreased from 37% in 2009 (102.7 versus 64.8) to 20% in 2014 (237.8 versus 191.3). The relative difference in BRCA testing rates between metropolitan and nonmetropolitan areas decreased more over time in younger women than in older women and decreased in all regions except the West. Receipt of preventive services 90 days after BRCA testing in metropolitan versus nonmetropolitan areas throughout the period varied by service: the percentage of women who received a mastectomy was similar, the percentage of women who received magnetic resonance imaging of the breast was lower in nonmetropolitan areas (as low as 5.8% in 2014 to as high as 8.2% in 2011) than metropolitan areas (as low as 7.3% in 2014 to as high as 10.3% in 2011), and the percentage of women who received mammography was lower in nonmetropolitan areas in earlier years but was similar in later years.
Interpretation: Possible explanations for the 47% decrease in the relative difference in BRCA testing rates over the study period include increased access to genetic services in nonmetropolitan areas and increased demand nationally as a result of publicity. The relative differences in metropolitan and nonmetropolitan BRCA testing rates were smaller among women at younger ages compared with older ages.
Public health action: Improved data sources and surveillance tools are needed to gather comprehensive data on BRCA testing in the United States, monitor adherence to evidence-based guidelines for BRCA testing, and assess receipt of preventive interventions for women with BRCA mutations. Programs can build on the recent decrease in geographic disparities in receipt of BRCA testing while simultaneously educating the public and health care providers about U.S. Preventive Services Task Force recommendations and other clinical guidelines for BRCA testing and counseling.
期刊介绍:
The Morbidity and Mortality Weekly Report (MMWR) Series, produced by the Centers for Disease Control and Prevention (CDC), is commonly referred to as "the voice of CDC." Serving as the primary outlet for timely, reliable, authoritative, accurate, objective, and practical public health information and recommendations, the MMWR is a crucial publication. Its readership primarily includes physicians, nurses, public health practitioners, epidemiologists, scientists, researchers, educators, and laboratorians.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
