Salika M Shakir, Margaret V Powers-Fletcher, E Susan Slechta, Mark A Fisher
{"title":"终末期肾病患者的犬幽门螺杆菌菌血症和蜂窝织炎","authors":"Salika M Shakir, Margaret V Powers-Fletcher, E Susan Slechta, Mark A Fisher","doi":"10.1099/jmmcr.0.005126","DOIUrl":null,"url":null,"abstract":"<p><p><b>Introduction.</b> Invasive infections by <i>Helicobacter canis</i> are uncommon and occur primarily in immunocompromised patients. Here, we describe a case of <i>H. canis</i> bacteraemia and cellulitis in a patient with end-stage renal disease (ESRD). <b>Case presentation.</b> A 49-year-old male with ESRD on haemodialysis presented to an emergency department with cellulitis overlying his left upper extremity arteriovenous fistula for 3 days without constitutional symptoms. Mild leucocytosis and thrombocytopenia was noted on initial laboratory work up. The patient received a dose of vancomycin initially, and then transitioned to oral doxycycline prior to discharge 3 days later. Blood cultures drawn on admission were positive with curved Gram-negative rods at day 5. Routine sub-cultures initially failed to isolate the organism; however, small, tan colonies were observed on sheep blood agar incubated under microaerobic conditions. <i>H. canis</i> was identified by 16S rRNA sequencing. Antimicrobial-susceptibility testing was not performed due to poor growth and lack of interpretive guidelines. The patient was ultimately treated successfully with amoxicillin/clavulanic acid. <b>Conclusion.</b> This case illustrates the importance of recognizing <i>H. canis</i> infections in immunocompromised patients, especially in those with recent pet exposure. In addition, this case highlights the need for improved laboratory diagnostics for <i>H. canis</i> as isolation and identification of this fastidious organism is challenging.</p>","PeriodicalId":73559,"journal":{"name":"JMM case reports","volume":"4 11","pages":"e005126"},"PeriodicalIF":0.0000,"publicationDate":"2017-11-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5729898/pdf/","citationCount":"3","resultStr":"{\"title\":\"<i>Helicobacter canis</i> bacteraemia and cellulitis in a patient with end-stage renal disease.\",\"authors\":\"Salika M Shakir, Margaret V Powers-Fletcher, E Susan Slechta, Mark A Fisher\",\"doi\":\"10.1099/jmmcr.0.005126\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Introduction.</b> Invasive infections by <i>Helicobacter canis</i> are uncommon and occur primarily in immunocompromised patients. Here, we describe a case of <i>H. canis</i> bacteraemia and cellulitis in a patient with end-stage renal disease (ESRD). <b>Case presentation.</b> A 49-year-old male with ESRD on haemodialysis presented to an emergency department with cellulitis overlying his left upper extremity arteriovenous fistula for 3 days without constitutional symptoms. Mild leucocytosis and thrombocytopenia was noted on initial laboratory work up. The patient received a dose of vancomycin initially, and then transitioned to oral doxycycline prior to discharge 3 days later. Blood cultures drawn on admission were positive with curved Gram-negative rods at day 5. Routine sub-cultures initially failed to isolate the organism; however, small, tan colonies were observed on sheep blood agar incubated under microaerobic conditions. <i>H. canis</i> was identified by 16S rRNA sequencing. Antimicrobial-susceptibility testing was not performed due to poor growth and lack of interpretive guidelines. The patient was ultimately treated successfully with amoxicillin/clavulanic acid. <b>Conclusion.</b> This case illustrates the importance of recognizing <i>H. canis</i> infections in immunocompromised patients, especially in those with recent pet exposure. In addition, this case highlights the need for improved laboratory diagnostics for <i>H. canis</i> as isolation and identification of this fastidious organism is challenging.</p>\",\"PeriodicalId\":73559,\"journal\":{\"name\":\"JMM case reports\",\"volume\":\"4 11\",\"pages\":\"e005126\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2017-11-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5729898/pdf/\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMM case reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1099/jmmcr.0.005126\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/11/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMM case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1099/jmmcr.0.005126","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/11/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Helicobacter canis bacteraemia and cellulitis in a patient with end-stage renal disease.
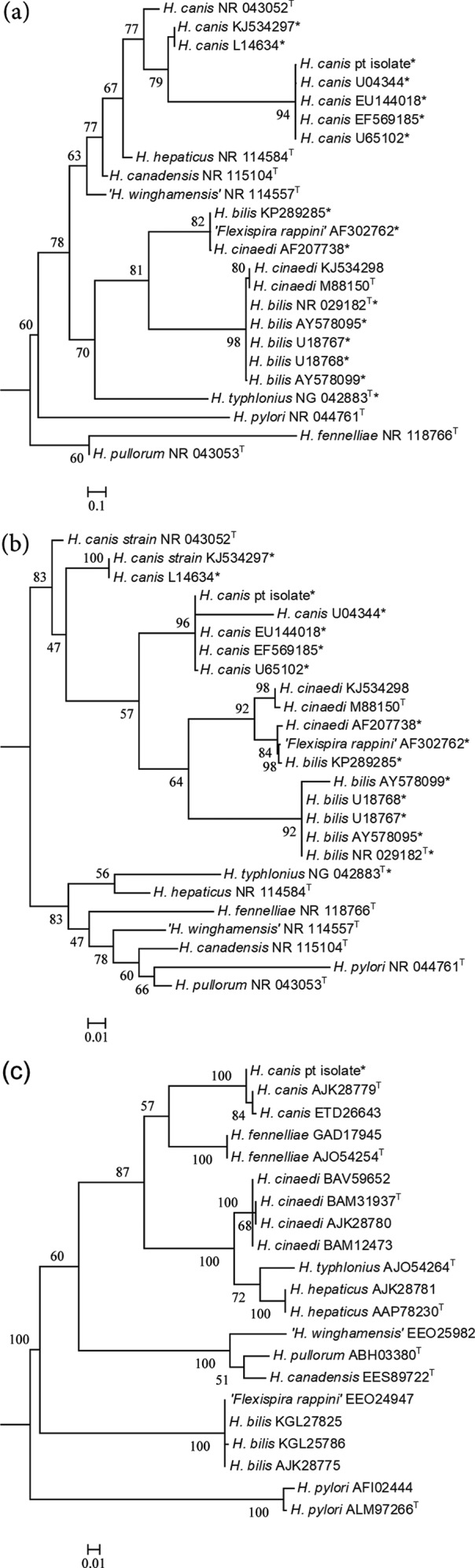
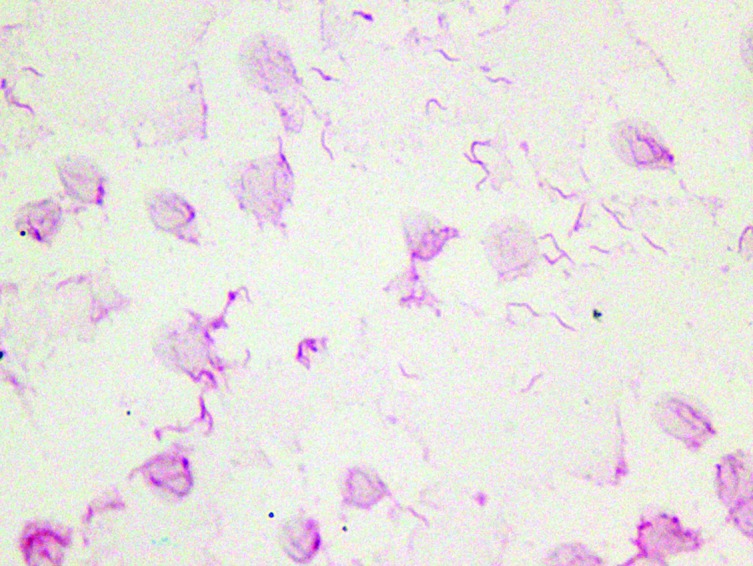
Introduction. Invasive infections by Helicobacter canis are uncommon and occur primarily in immunocompromised patients. Here, we describe a case of H. canis bacteraemia and cellulitis in a patient with end-stage renal disease (ESRD). Case presentation. A 49-year-old male with ESRD on haemodialysis presented to an emergency department with cellulitis overlying his left upper extremity arteriovenous fistula for 3 days without constitutional symptoms. Mild leucocytosis and thrombocytopenia was noted on initial laboratory work up. The patient received a dose of vancomycin initially, and then transitioned to oral doxycycline prior to discharge 3 days later. Blood cultures drawn on admission were positive with curved Gram-negative rods at day 5. Routine sub-cultures initially failed to isolate the organism; however, small, tan colonies were observed on sheep blood agar incubated under microaerobic conditions. H. canis was identified by 16S rRNA sequencing. Antimicrobial-susceptibility testing was not performed due to poor growth and lack of interpretive guidelines. The patient was ultimately treated successfully with amoxicillin/clavulanic acid. Conclusion. This case illustrates the importance of recognizing H. canis infections in immunocompromised patients, especially in those with recent pet exposure. In addition, this case highlights the need for improved laboratory diagnostics for H. canis as isolation and identification of this fastidious organism is challenging.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
