Uchenna Ekwochi, Nwabueze I Asinobi, Chidiebere DI Osuorah, Ikenna K Ndu, Christian Ifediora, Ogechukwu F Amadi, Chukwunonso C Iheji, Casmir Jg Orjioke, Wilfred O Okenwa, Bernadette Ifeyinwa Okeke
{"title":"围产期窒息新生儿死亡率的发病率和预测因素:尼日利亚东南部埃努古卫生保健机构新生儿4年前瞻性研究","authors":"Uchenna Ekwochi, Nwabueze I Asinobi, Chidiebere DI Osuorah, Ikenna K Ndu, Christian Ifediora, Ogechukwu F Amadi, Chukwunonso C Iheji, Casmir Jg Orjioke, Wilfred O Okenwa, Bernadette Ifeyinwa Okeke","doi":"10.1177/1179556517746646","DOIUrl":null,"url":null,"abstract":"<p><p>Fatalities from perinatal asphyxia remain high in developing countries, and continually assessing its risk factors will help improve outcomes in these settings. We explored how some identified risk factors predict mortality in asphyxiated newborns, to assist clinicians in prioritizing interventions. This was a 4-year prospective study conducted at the Enugu State University Teaching Hospital, Enugu, Nigeria. All newborns who met the study criteria that were admitted to this facility in this period were enrolled and monitored. Data collected were analysed with SPSS Version 18. A total of 161 newborns with perinatal asphyxia were enrolled into the study with an in-hospital incidence rate of 12.81 per 1000 birth and a case fatality rate of 18%. Overall, the APGAR scores were severe in 10%, moderate in 22%, mild to normal in 68%, whereas the SARNAT stages were III in 24%, II in 52%, and I in 25%. In terms of mortality, 66.7%, 22.2%, and 11.1% mortalities were, respectively, observed with SARNAT scores III, II, and I (<i>P </i>= .003), whereas the findings with APGAR were 31.2% (severe), 25.0% (moderate), 25.0% (mild), and 18.8% (normal) (<i>P </i>= .030). Fatality outcome was more correlated with SARNAT (<i>R </i>= .280; <i>P </i>= .000) than APGAR (<i>R </i>= -.247; <i>P </i>= .0125). The SARNAT score significantly differentiated between the degrees of asphyxia in newborns based on gestational age at delivery (<i>P </i>= .010), place of delivery (<i>P </i>= .032), and mode of delivery (<i>P </i>= .042). Finally, it was noted that newborns that were female (<i>P </i>= .007), or born outside the hospital (<i>P </i>= .010), or with oxygen saturations <60% (<i>P </i>= .001), or with heart rate <120 (<i>P </i>= .000), and those with respiratory rate <30 (<i>P </i>= .003), all have significantly higher likelihood of deaths from asphyxia. Therefore, predictors of neonatal mortality from perinatal asphyxia in our centre include being female and being born outside the hospital, as well as low oxygen saturations, heart rates, and respiratory rates at presentation.</p>","PeriodicalId":45027,"journal":{"name":"Clinical Medicine Insights-Pediatrics","volume":"11 ","pages":"1179556517746646"},"PeriodicalIF":1.2000,"publicationDate":"2017-12-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1179556517746646","citationCount":"22","resultStr":"{\"title\":\"Incidence and Predictors of Mortality Among Newborns With Perinatal Asphyxia: A 4-Year Prospective Study of Newborns Delivered in Health Care Facilities in Enugu, South-East Nigeria.\",\"authors\":\"Uchenna Ekwochi, Nwabueze I Asinobi, Chidiebere DI Osuorah, Ikenna K Ndu, Christian Ifediora, Ogechukwu F Amadi, Chukwunonso C Iheji, Casmir Jg Orjioke, Wilfred O Okenwa, Bernadette Ifeyinwa Okeke\",\"doi\":\"10.1177/1179556517746646\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Fatalities from perinatal asphyxia remain high in developing countries, and continually assessing its risk factors will help improve outcomes in these settings. We explored how some identified risk factors predict mortality in asphyxiated newborns, to assist clinicians in prioritizing interventions. This was a 4-year prospective study conducted at the Enugu State University Teaching Hospital, Enugu, Nigeria. All newborns who met the study criteria that were admitted to this facility in this period were enrolled and monitored. Data collected were analysed with SPSS Version 18. A total of 161 newborns with perinatal asphyxia were enrolled into the study with an in-hospital incidence rate of 12.81 per 1000 birth and a case fatality rate of 18%. Overall, the APGAR scores were severe in 10%, moderate in 22%, mild to normal in 68%, whereas the SARNAT stages were III in 24%, II in 52%, and I in 25%. In terms of mortality, 66.7%, 22.2%, and 11.1% mortalities were, respectively, observed with SARNAT scores III, II, and I (<i>P </i>= .003), whereas the findings with APGAR were 31.2% (severe), 25.0% (moderate), 25.0% (mild), and 18.8% (normal) (<i>P </i>= .030). Fatality outcome was more correlated with SARNAT (<i>R </i>= .280; <i>P </i>= .000) than APGAR (<i>R </i>= -.247; <i>P </i>= .0125). The SARNAT score significantly differentiated between the degrees of asphyxia in newborns based on gestational age at delivery (<i>P </i>= .010), place of delivery (<i>P </i>= .032), and mode of delivery (<i>P </i>= .042). Finally, it was noted that newborns that were female (<i>P </i>= .007), or born outside the hospital (<i>P </i>= .010), or with oxygen saturations <60% (<i>P </i>= .001), or with heart rate <120 (<i>P </i>= .000), and those with respiratory rate <30 (<i>P </i>= .003), all have significantly higher likelihood of deaths from asphyxia. Therefore, predictors of neonatal mortality from perinatal asphyxia in our centre include being female and being born outside the hospital, as well as low oxygen saturations, heart rates, and respiratory rates at presentation.</p>\",\"PeriodicalId\":45027,\"journal\":{\"name\":\"Clinical Medicine Insights-Pediatrics\",\"volume\":\"11 \",\"pages\":\"1179556517746646\"},\"PeriodicalIF\":1.2000,\"publicationDate\":\"2017-12-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1179556517746646\",\"citationCount\":\"22\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Medicine Insights-Pediatrics\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1179556517746646\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2017/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179556517746646","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PEDIATRICS","Score":null,"Total":0}
Incidence and Predictors of Mortality Among Newborns With Perinatal Asphyxia: A 4-Year Prospective Study of Newborns Delivered in Health Care Facilities in Enugu, South-East Nigeria.
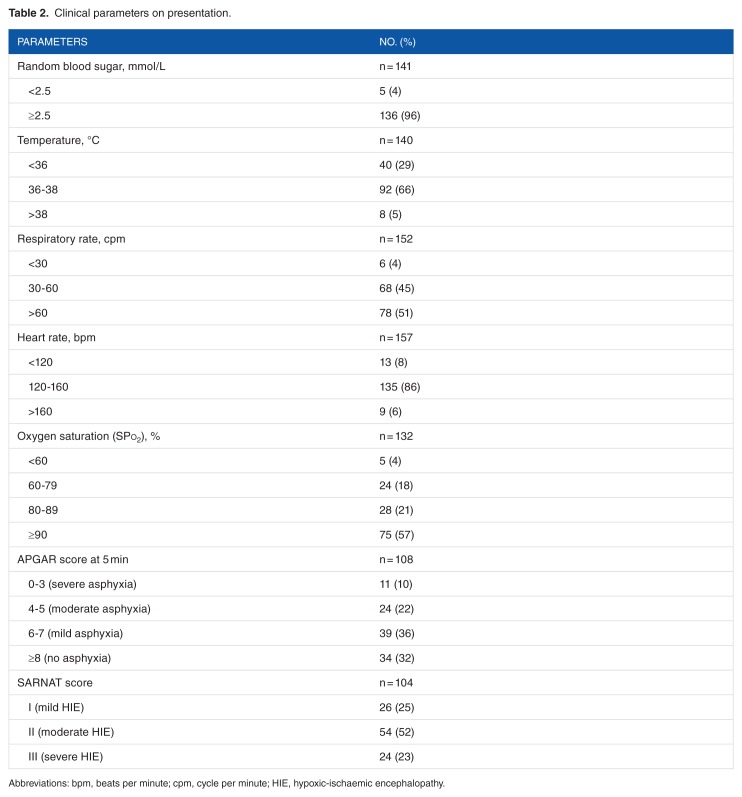
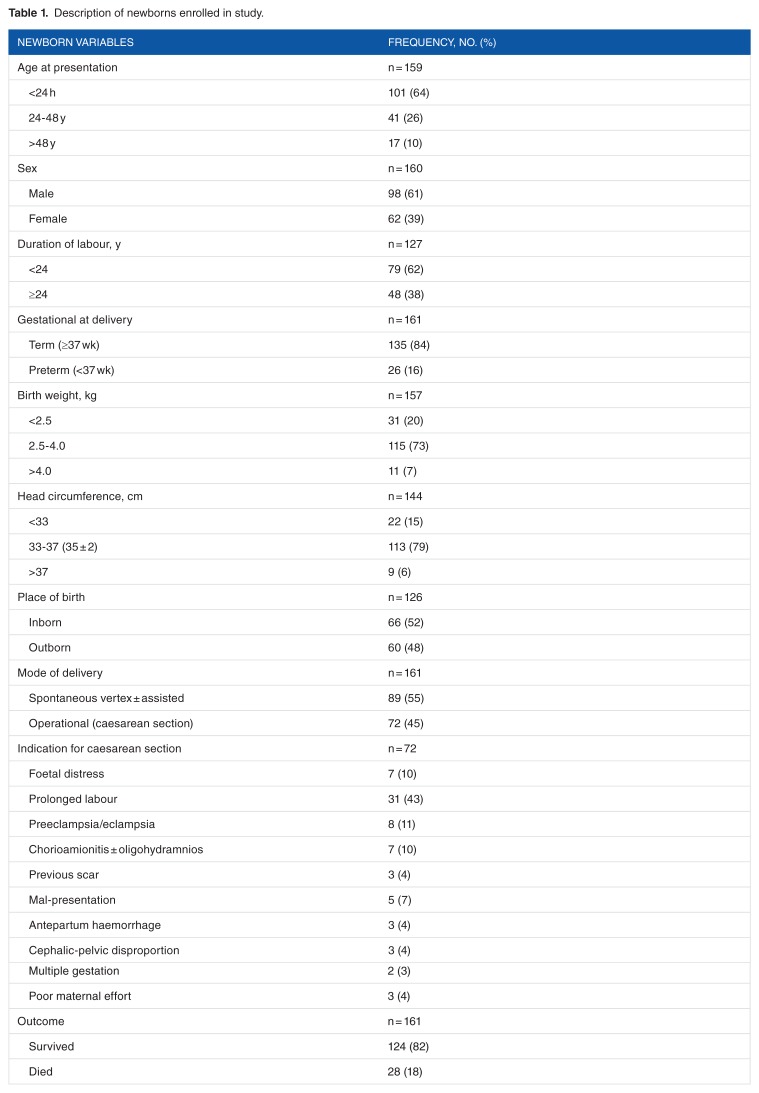
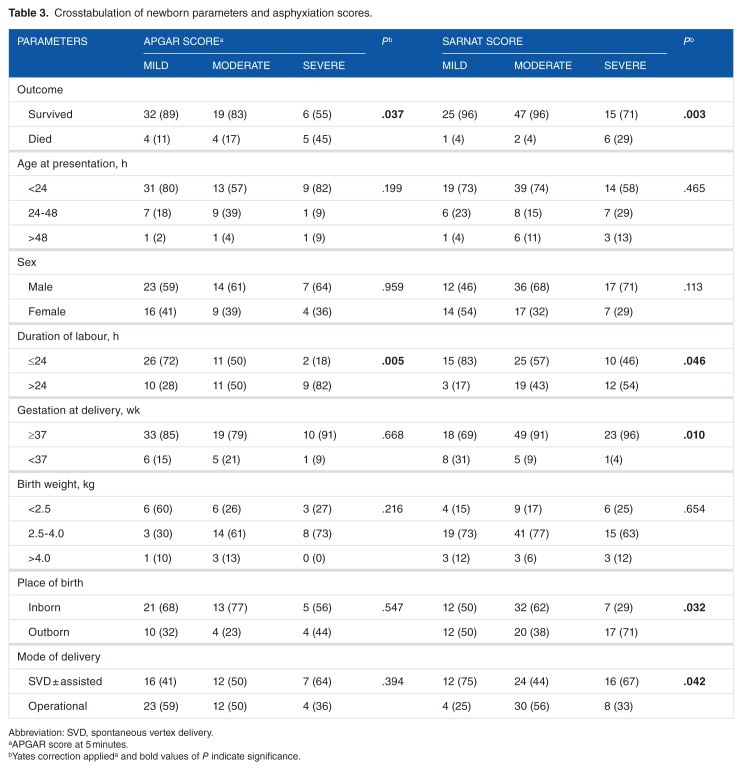
Fatalities from perinatal asphyxia remain high in developing countries, and continually assessing its risk factors will help improve outcomes in these settings. We explored how some identified risk factors predict mortality in asphyxiated newborns, to assist clinicians in prioritizing interventions. This was a 4-year prospective study conducted at the Enugu State University Teaching Hospital, Enugu, Nigeria. All newborns who met the study criteria that were admitted to this facility in this period were enrolled and monitored. Data collected were analysed with SPSS Version 18. A total of 161 newborns with perinatal asphyxia were enrolled into the study with an in-hospital incidence rate of 12.81 per 1000 birth and a case fatality rate of 18%. Overall, the APGAR scores were severe in 10%, moderate in 22%, mild to normal in 68%, whereas the SARNAT stages were III in 24%, II in 52%, and I in 25%. In terms of mortality, 66.7%, 22.2%, and 11.1% mortalities were, respectively, observed with SARNAT scores III, II, and I (P = .003), whereas the findings with APGAR were 31.2% (severe), 25.0% (moderate), 25.0% (mild), and 18.8% (normal) (P = .030). Fatality outcome was more correlated with SARNAT (R = .280; P = .000) than APGAR (R = -.247; P = .0125). The SARNAT score significantly differentiated between the degrees of asphyxia in newborns based on gestational age at delivery (P = .010), place of delivery (P = .032), and mode of delivery (P = .042). Finally, it was noted that newborns that were female (P = .007), or born outside the hospital (P = .010), or with oxygen saturations <60% (P = .001), or with heart rate <120 (P = .000), and those with respiratory rate <30 (P = .003), all have significantly higher likelihood of deaths from asphyxia. Therefore, predictors of neonatal mortality from perinatal asphyxia in our centre include being female and being born outside the hospital, as well as low oxygen saturations, heart rates, and respiratory rates at presentation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
