Joe Littlechild, Muneer Junejo, Anne-Marie Simons, Finlay Curran, Darren Subar
{"title":"结直肠癌急诊切除手术:疾病复发和生存模式。","authors":"Joe Littlechild, Muneer Junejo, Anne-Marie Simons, Finlay Curran, Darren Subar","doi":"10.4291/wjgp.v9.i1.8","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>To evaluate prognostic pathological factors associated with early metachronous disease and adverse long-term survival in these patients.</p><p><strong>Methods: </strong>Clinical and histological features were analysed retrospectively over an eight-year period for prognostic impact on recurrent disease and overall survival in patients undergoing curative resection of a primary colorectal cancer.</p><p><strong>Results: </strong>A total of 266 patients underwent curative surgery during the study period. The median age of the study cohort was 68 year (range 26 to 91) with a follow-up of 7.9 years (range 4.6 to 12.6). Resection was undertaken electively in 225 (84.6%) patients and emergency resection in 35 (13.2%). Data on timing of surgery was missing in 6 patients. Recurrence was noted in 67 (25.2%) during the study period and was predominantly early within 3 years (82.1%) and involved hepatic metastasis in 73.1%. Emergency resection (OR = 3.60, <i>P</i> = 0.001), T4 stage (OR = 4.33, <i>P</i> < 0.001) and lymphovascular invasion (LVI) (OR = 2.37, <i>P</i> = 0.032) were associated with higher risk of recurrent disease. Emergency resection, T4 disease and a high lymph node ratio (LNR) were strong independent predictors of adverse long-term survival.</p><p><strong>Conclusion: </strong>Emergency surgery is associated with adverse disease free and long-term survival. T4 disease, LVI and LNR provide strong independent predictive value of long-term outcome and can inform surveillance strategies to improve outcomes.</p>","PeriodicalId":23760,"journal":{"name":"World Journal of Gastrointestinal Pathophysiology","volume":"9 1","pages":"8-17"},"PeriodicalIF":0.0000,"publicationDate":"2018-02-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bf/8e/WJGP-9-8.PMC5823701.pdf","citationCount":"10","resultStr":"{\"title\":\"Emergency resection surgery for colorectal cancer: Patterns of recurrent disease and survival.\",\"authors\":\"Joe Littlechild, Muneer Junejo, Anne-Marie Simons, Finlay Curran, Darren Subar\",\"doi\":\"10.4291/wjgp.v9.i1.8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aim: </strong>To evaluate prognostic pathological factors associated with early metachronous disease and adverse long-term survival in these patients.</p><p><strong>Methods: </strong>Clinical and histological features were analysed retrospectively over an eight-year period for prognostic impact on recurrent disease and overall survival in patients undergoing curative resection of a primary colorectal cancer.</p><p><strong>Results: </strong>A total of 266 patients underwent curative surgery during the study period. The median age of the study cohort was 68 year (range 26 to 91) with a follow-up of 7.9 years (range 4.6 to 12.6). Resection was undertaken electively in 225 (84.6%) patients and emergency resection in 35 (13.2%). Data on timing of surgery was missing in 6 patients. Recurrence was noted in 67 (25.2%) during the study period and was predominantly early within 3 years (82.1%) and involved hepatic metastasis in 73.1%. Emergency resection (OR = 3.60, <i>P</i> = 0.001), T4 stage (OR = 4.33, <i>P</i> < 0.001) and lymphovascular invasion (LVI) (OR = 2.37, <i>P</i> = 0.032) were associated with higher risk of recurrent disease. Emergency resection, T4 disease and a high lymph node ratio (LNR) were strong independent predictors of adverse long-term survival.</p><p><strong>Conclusion: </strong>Emergency surgery is associated with adverse disease free and long-term survival. T4 disease, LVI and LNR provide strong independent predictive value of long-term outcome and can inform surveillance strategies to improve outcomes.</p>\",\"PeriodicalId\":23760,\"journal\":{\"name\":\"World Journal of Gastrointestinal Pathophysiology\",\"volume\":\"9 1\",\"pages\":\"8-17\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2018-02-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bf/8e/WJGP-9-8.PMC5823701.pdf\",\"citationCount\":\"10\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Gastrointestinal Pathophysiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4291/wjgp.v9.i1.8\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Pathophysiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4291/wjgp.v9.i1.8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 10
摘要
目的:评价与早期异时性疾病相关的预后病理因素和不良的长期生存。方法:回顾性分析原发性结直肠癌根治性切除术患者的临床和组织学特征对复发疾病和总生存期的预后影响。结果:研究期间共有266例患者接受了根治性手术。研究队列的中位年龄为68岁(26 - 91岁),随访7.9年(4.6 - 12.6年)。选择性切除225例(84.6%),急诊切除35例(13.2%)。6例患者手术时间资料缺失。在研究期间有67例(25.2%)复发,主要是3年内早期复发(82.1%),73.1%伴有肝转移。急诊切除(OR = 3.60, P = 0.001)、T4期(OR = 4.33, P < 0.001)和淋巴血管侵犯(LVI) (OR = 2.37, P = 0.032)与较高的复发风险相关。急诊切除、T4病变和高淋巴结率(LNR)是不良长期生存的独立预测因素。结论:急诊手术与无不良疾病和长期生存相关。T4疾病、LVI和LNR为长期预后提供了强大的独立预测价值,可以为改善预后的监测策略提供信息。
Emergency resection surgery for colorectal cancer: Patterns of recurrent disease and survival.
Aim: To evaluate prognostic pathological factors associated with early metachronous disease and adverse long-term survival in these patients.
Methods: Clinical and histological features were analysed retrospectively over an eight-year period for prognostic impact on recurrent disease and overall survival in patients undergoing curative resection of a primary colorectal cancer.
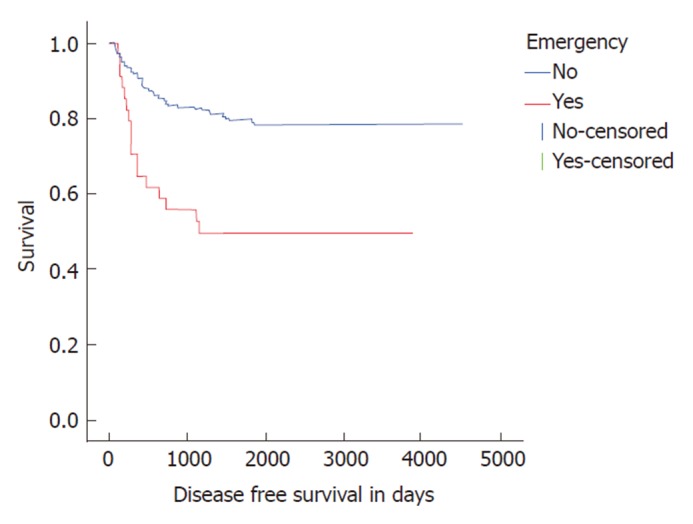
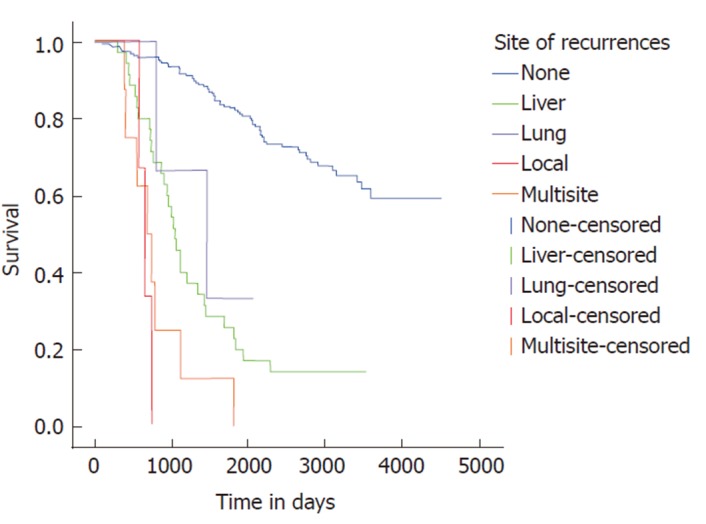
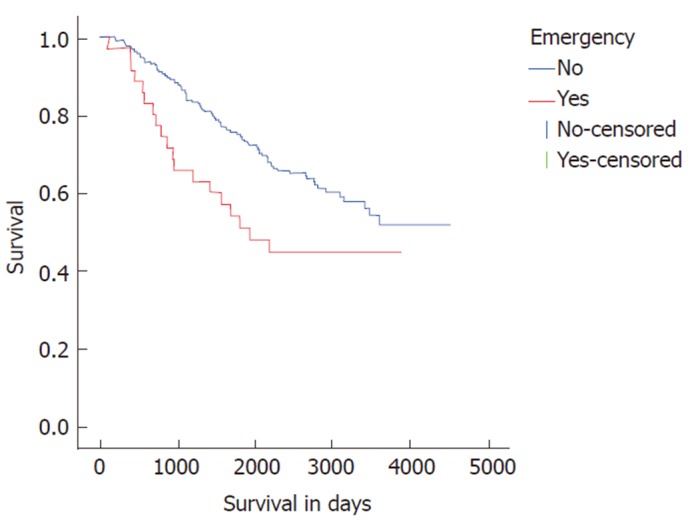
Results: A total of 266 patients underwent curative surgery during the study period. The median age of the study cohort was 68 year (range 26 to 91) with a follow-up of 7.9 years (range 4.6 to 12.6). Resection was undertaken electively in 225 (84.6%) patients and emergency resection in 35 (13.2%). Data on timing of surgery was missing in 6 patients. Recurrence was noted in 67 (25.2%) during the study period and was predominantly early within 3 years (82.1%) and involved hepatic metastasis in 73.1%. Emergency resection (OR = 3.60, P = 0.001), T4 stage (OR = 4.33, P < 0.001) and lymphovascular invasion (LVI) (OR = 2.37, P = 0.032) were associated with higher risk of recurrent disease. Emergency resection, T4 disease and a high lymph node ratio (LNR) were strong independent predictors of adverse long-term survival.
Conclusion: Emergency surgery is associated with adverse disease free and long-term survival. T4 disease, LVI and LNR provide strong independent predictive value of long-term outcome and can inform surveillance strategies to improve outcomes.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
