T Benkö, M Gottmann, S Radunz, A Bienholz, F H Saner, J W Treckmann, A Paul, D P Hoyer
{"title":"移植时接受抗血小板治疗的肾移植受者一年同种异体移植和患者生存率。","authors":"T Benkö, M Gottmann, S Radunz, A Bienholz, F H Saner, J W Treckmann, A Paul, D P Hoyer","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Antiplatelet therapy is common in patients on the waiting list for kidney transplantation.</p><p><strong>Objective: </strong>To evaluate the incidence of post-operative bleeding in patients with antiplatelet therapy undergoing kidney transplantation and analyze the impact on the outcome.</p><p><strong>Methods: </strong>We studied all patients with concomitant antiplatelet therapy undergoing kidney transplantation in our center from January 2007 to June 2012. Data were collected by chart review. Univariate and multivariate logistic regression and Cox proportional hazard model were used to identify risk factors for the long-term outcome.</p><p><strong>Results: </strong>Of 744 kidney transplant recipients during the study period, 161 received oral antiplatelet therapy and were included in the study. One-third of the patients demonstrated signs of bleeding, half of which requiring surgical treatment. Coronary artery disease, deceased donor kidney transplantation, and dual antiplatelet medication were independent risk factors for post-operative bleeding. One-year allograft survival was significantly better in the non-bleeding group (91.4% <i>vs</i> 75.9%, p=0.023). Multivariable analysis found that post-operative bleeding, recipient age, and biopsy-proven rejection were independent risk factors for graft survival. Recipient age and biopsy-proven rejection were also identified as independent risk factors for patient survival.</p><p><strong>Conclusion: </strong>This analysis indicated a high risk for post-operative bleeding in renal transplant patients under antiplatelet therapy. The associated negative effect on allograft survival underscored the need to reduce any risk factors for post-operative bleeding.</p>","PeriodicalId":14242,"journal":{"name":"International Journal of Organ Transplantation Medicine","volume":"9 1","pages":"10-19"},"PeriodicalIF":0.2000,"publicationDate":"2018-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5839625/pdf/","citationCount":"0","resultStr":"{\"title\":\"One-year Allograft and Patient Survival in Renal Transplant Recipients Receiving Antiplatelet Therapy at the Time of Transplantation.\",\"authors\":\"T Benkö, M Gottmann, S Radunz, A Bienholz, F H Saner, J W Treckmann, A Paul, D P Hoyer\",\"doi\":\"\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Antiplatelet therapy is common in patients on the waiting list for kidney transplantation.</p><p><strong>Objective: </strong>To evaluate the incidence of post-operative bleeding in patients with antiplatelet therapy undergoing kidney transplantation and analyze the impact on the outcome.</p><p><strong>Methods: </strong>We studied all patients with concomitant antiplatelet therapy undergoing kidney transplantation in our center from January 2007 to June 2012. Data were collected by chart review. Univariate and multivariate logistic regression and Cox proportional hazard model were used to identify risk factors for the long-term outcome.</p><p><strong>Results: </strong>Of 744 kidney transplant recipients during the study period, 161 received oral antiplatelet therapy and were included in the study. One-third of the patients demonstrated signs of bleeding, half of which requiring surgical treatment. Coronary artery disease, deceased donor kidney transplantation, and dual antiplatelet medication were independent risk factors for post-operative bleeding. One-year allograft survival was significantly better in the non-bleeding group (91.4% <i>vs</i> 75.9%, p=0.023). Multivariable analysis found that post-operative bleeding, recipient age, and biopsy-proven rejection were independent risk factors for graft survival. Recipient age and biopsy-proven rejection were also identified as independent risk factors for patient survival.</p><p><strong>Conclusion: </strong>This analysis indicated a high risk for post-operative bleeding in renal transplant patients under antiplatelet therapy. The associated negative effect on allograft survival underscored the need to reduce any risk factors for post-operative bleeding.</p>\",\"PeriodicalId\":14242,\"journal\":{\"name\":\"International Journal of Organ Transplantation Medicine\",\"volume\":\"9 1\",\"pages\":\"10-19\"},\"PeriodicalIF\":0.2000,\"publicationDate\":\"2018-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5839625/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Organ Transplantation Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/2/1 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"TRANSPLANTATION\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Organ Transplantation Medicine","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/2/1 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
摘要
背景:抗血小板治疗在等待肾移植的患者中很常见。目的:评价肾移植术后接受抗血小板治疗的患者术后出血的发生率,并分析其对预后的影响。方法:对2007年1月至2012年6月在我中心接受肾移植同时抗血小板治疗的患者进行研究。通过图表回顾收集数据。采用单因素和多因素logistic回归及Cox比例风险模型确定影响长期预后的危险因素。结果:在研究期间的744例肾移植受者中,有161例接受了口服抗血小板治疗,并被纳入研究。三分之一的患者表现出出血的迹象,其中一半需要手术治疗。冠状动脉疾病、死亡供肾移植和双重抗血小板药物是术后出血的独立危险因素。非出血组一年同种异体移植存活率显著提高(91.4% vs 75.9%, p=0.023)。多变量分析发现,术后出血、受体年龄和活检证实的排斥反应是移植物存活的独立危险因素。受体年龄和活检证实的排斥反应也被确定为患者生存的独立危险因素。结论:本分析提示肾移植术后接受抗血小板治疗的患者出血风险高。对同种异体移植存活的相关负面影响强调了减少术后出血的任何危险因素的必要性。
One-year Allograft and Patient Survival in Renal Transplant Recipients Receiving Antiplatelet Therapy at the Time of Transplantation.
Background: Antiplatelet therapy is common in patients on the waiting list for kidney transplantation.
Objective: To evaluate the incidence of post-operative bleeding in patients with antiplatelet therapy undergoing kidney transplantation and analyze the impact on the outcome.
Methods: We studied all patients with concomitant antiplatelet therapy undergoing kidney transplantation in our center from January 2007 to June 2012. Data were collected by chart review. Univariate and multivariate logistic regression and Cox proportional hazard model were used to identify risk factors for the long-term outcome.
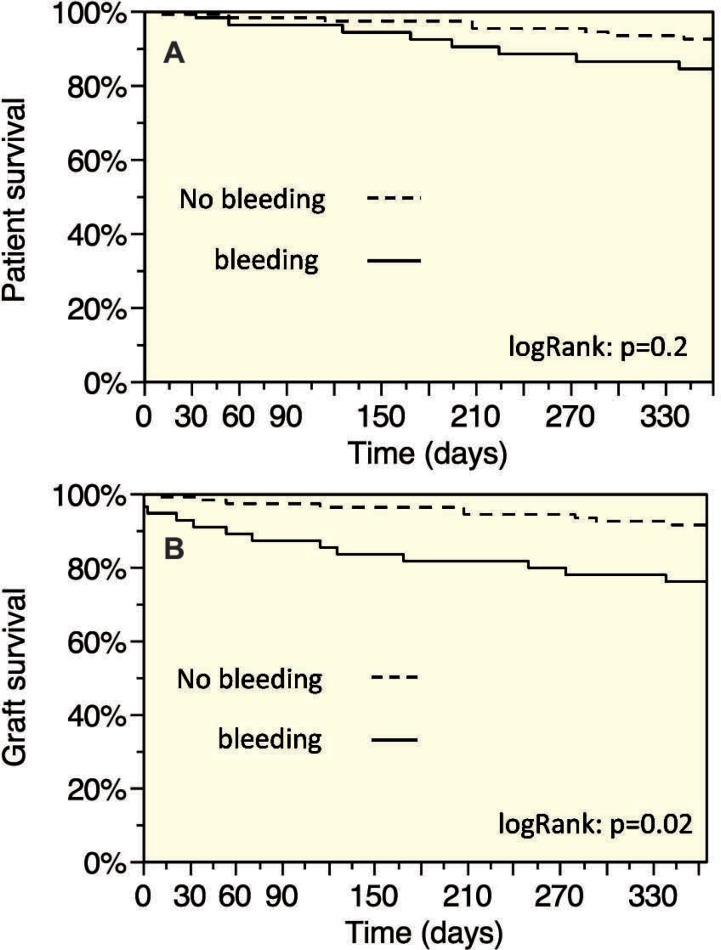
Results: Of 744 kidney transplant recipients during the study period, 161 received oral antiplatelet therapy and were included in the study. One-third of the patients demonstrated signs of bleeding, half of which requiring surgical treatment. Coronary artery disease, deceased donor kidney transplantation, and dual antiplatelet medication were independent risk factors for post-operative bleeding. One-year allograft survival was significantly better in the non-bleeding group (91.4% vs 75.9%, p=0.023). Multivariable analysis found that post-operative bleeding, recipient age, and biopsy-proven rejection were independent risk factors for graft survival. Recipient age and biopsy-proven rejection were also identified as independent risk factors for patient survival.
Conclusion: This analysis indicated a high risk for post-operative bleeding in renal transplant patients under antiplatelet therapy. The associated negative effect on allograft survival underscored the need to reduce any risk factors for post-operative bleeding.
期刊介绍:
The International Journal of Organ Transplantation Medicine (IJOTM) is a quarterly peer-reviewed English-language journal that publishes high-quality basic sciences and clinical research on transplantation. The scope of the journal includes organ and tissue donation, procurement and preservation; surgical techniques, innovations, and novelties in all aspects of transplantation; genomics and immunobiology; immunosuppressive drugs and pharmacology relevant to transplantation; graft survival and prevention of graft dysfunction and failure; clinical trials and population analyses in the field of transplantation; transplant complications; cell and tissue transplantation; infection; post-transplant malignancies; sociological and ethical issues and xenotransplantation.
 分享
分享




 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
