Eva O Melin, Hans O Thulesius, Magnus Hillman, Mona Landin-Olsson, Maria Thunander
{"title":"1型糖尿病腹部肥胖与性别、心血管危险因素和并发症以及实现治疗目标的困难相关:一项二级保健糖尿病诊所的横断面研究","authors":"Eva O Melin, Hans O Thulesius, Magnus Hillman, Mona Landin-Olsson, Maria Thunander","doi":"10.1186/s40608-018-0193-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Abdominal obesity is linked to cardiovascular diseases in type 1 diabetes (T1D). The primary aim was to explore associations between abdominal obesity and cardiovascular complications, metabolic and inflammatory factors. The secondary aim was to explore whether achieved recommended treatment targets differed between the obese and non-obese participants.</p><p><strong>Methods: </strong>Cross sectional study of 284 T1D patients (age 18-59 years, men 56%), consecutively recruited from one secondary care specialist diabetes clinic in Sweden. Anthropometrics, blood pressure, serum-lipids and high-sensitivity C-reactive protein (hs-CRP) were collected and supplemented with data from the patients' medical records and from the Swedish National Diabetes Registry. Abdominal obesity was defined as waist circumference men/women (meters): ≥1.02/≥0.88. Hs-CRP was divided into low-, moderate-, and high-risk groups for future cardiovascular events (< 1, 1 to 3, and > 3 to ≤8.9 mg/l). Treatment targets were blood pressure ≤ 130/≤ 80, total cholesterol ≤4.5 mmol/l, LDL: ≤ 2.5 mmol/l, and HbA1c: ≤5 2 mmol/mol (≤ 6.9%). Different explanatory linear, logistic and ordinal regression models were elaborated for the associations, and calibrated and validated for goodness of fit with the data variables.</p><p><strong>Results: </strong>The prevalence of abdominal obesity was 49/284 (17%), men/women: 8%/29% (<i>P</i> < 0.001). Women (adjusted odds ratio (AOR) 6.5), cardiovascular complications (AOR 5.7), HbA1c > 70 mmol/mol (> 8.6%) (AOR 2.7), systolic blood pressure (per mm Hg) (AOR 1.05), and triglycerides (per mmol/l) (AOR 1.7), were associated with abdominal obesity. Sub analyses (<i>n</i> = 171), showed that abdominal obesity (AOR 5.3) and triglycerides (per mmol/l) (AOR 2.8) were associated with increasing risk levels of hs-CRP. Treatment targets were obtained for fewer patients with abdominal obesity for HbA1c (8% vs 21%, <i>P</i> = 0.044) and systolic blood pressure (51% vs 68%, <i>P</i> = 0.033). No patients with abdominal obesity reached all treatment targets compared to 8% in patients without abdominal obesity.</p><p><strong>Conclusions: </strong>Significant associations between abdominal obesity and gender, cardiovascular disease, and the cardiovascular risk factors low-grade inflammation, systolic blood pressure, high HbA1c, and triglycerides, were found in 284 T1D patients. Fewer patients with abdominal obesity reached the treatment targets for HbA1c and systolic blood pressure compared to the non-obese.</p>","PeriodicalId":37440,"journal":{"name":"BMC Obesity","volume":"5 ","pages":"15"},"PeriodicalIF":0.0000,"publicationDate":"2018-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s40608-018-0193-5","citationCount":"27","resultStr":"{\"title\":\"Abdominal obesity in type 1 diabetes associated with gender, cardiovascular risk factors and complications, and difficulties achieving treatment targets: a cross sectional study at a secondary care diabetes clinic.\",\"authors\":\"Eva O Melin, Hans O Thulesius, Magnus Hillman, Mona Landin-Olsson, Maria Thunander\",\"doi\":\"10.1186/s40608-018-0193-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Abdominal obesity is linked to cardiovascular diseases in type 1 diabetes (T1D). The primary aim was to explore associations between abdominal obesity and cardiovascular complications, metabolic and inflammatory factors. The secondary aim was to explore whether achieved recommended treatment targets differed between the obese and non-obese participants.</p><p><strong>Methods: </strong>Cross sectional study of 284 T1D patients (age 18-59 years, men 56%), consecutively recruited from one secondary care specialist diabetes clinic in Sweden. Anthropometrics, blood pressure, serum-lipids and high-sensitivity C-reactive protein (hs-CRP) were collected and supplemented with data from the patients' medical records and from the Swedish National Diabetes Registry. Abdominal obesity was defined as waist circumference men/women (meters): ≥1.02/≥0.88. Hs-CRP was divided into low-, moderate-, and high-risk groups for future cardiovascular events (< 1, 1 to 3, and > 3 to ≤8.9 mg/l). Treatment targets were blood pressure ≤ 130/≤ 80, total cholesterol ≤4.5 mmol/l, LDL: ≤ 2.5 mmol/l, and HbA1c: ≤5 2 mmol/mol (≤ 6.9%). Different explanatory linear, logistic and ordinal regression models were elaborated for the associations, and calibrated and validated for goodness of fit with the data variables.</p><p><strong>Results: </strong>The prevalence of abdominal obesity was 49/284 (17%), men/women: 8%/29% (<i>P</i> < 0.001). Women (adjusted odds ratio (AOR) 6.5), cardiovascular complications (AOR 5.7), HbA1c > 70 mmol/mol (> 8.6%) (AOR 2.7), systolic blood pressure (per mm Hg) (AOR 1.05), and triglycerides (per mmol/l) (AOR 1.7), were associated with abdominal obesity. Sub analyses (<i>n</i> = 171), showed that abdominal obesity (AOR 5.3) and triglycerides (per mmol/l) (AOR 2.8) were associated with increasing risk levels of hs-CRP. Treatment targets were obtained for fewer patients with abdominal obesity for HbA1c (8% vs 21%, <i>P</i> = 0.044) and systolic blood pressure (51% vs 68%, <i>P</i> = 0.033). No patients with abdominal obesity reached all treatment targets compared to 8% in patients without abdominal obesity.</p><p><strong>Conclusions: </strong>Significant associations between abdominal obesity and gender, cardiovascular disease, and the cardiovascular risk factors low-grade inflammation, systolic blood pressure, high HbA1c, and triglycerides, were found in 284 T1D patients. Fewer patients with abdominal obesity reached the treatment targets for HbA1c and systolic blood pressure compared to the non-obese.</p>\",\"PeriodicalId\":37440,\"journal\":{\"name\":\"BMC Obesity\",\"volume\":\"5 \",\"pages\":\"15\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2018-05-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s40608-018-0193-5\",\"citationCount\":\"27\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Obesity\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s40608-018-0193-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Obesity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40608-018-0193-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 27
摘要
背景:腹部肥胖与1型糖尿病(T1D)的心血管疾病有关。主要目的是探讨腹部肥胖与心血管并发症、代谢和炎症因素之间的关系。第二个目的是探讨肥胖和非肥胖参与者是否达到了推荐的治疗目标。方法:横断面研究284例T1D患者(年龄18-59岁,男性56%),从瑞典一家二级保健专科糖尿病诊所连续招募。收集人体测量、血压、血脂和高敏c反应蛋白(hs-CRP)数据,并辅以患者医疗记录和瑞典国家糖尿病登记处的数据。腹部肥胖定义为腰围男性/女性(米):≥1.02/≥0.88。Hs-CRP被分为未来心血管事件低、中、高危组(3 ~≤8.9 mg/l)。治疗目标为血压≤130/≤80,总胆固醇≤4.5 mmol/l, LDL≤2.5 mmol/l, HbA1c≤5.2 mmol/mol(≤6.9%)。不同的解释线性,逻辑和有序回归模型阐述了关联,并校准和验证了与数据变量的拟合优度。结果:腹部肥胖患病率为49/284(17%),男女患病率为8%/29% (P < 0.001)。女性(调整优势比(AOR) 6.5)、心血管并发症(AOR 5.7)、HbA1c > 70 mmol/mol (> 8.6%) (AOR 2.7)、收缩压(每毫米汞柱)(AOR 1.05)和甘油三酯(每mmol/l) (AOR 1.7)与腹部肥胖相关。亚组分析(n = 171)显示,腹部肥胖(AOR 5.3)和甘油三酯(每mmol/l) (AOR 2.8)与hs-CRP风险水平升高相关。较少腹部肥胖患者的治疗目标为HbA1c (8% vs 21%, P = 0.044)和收缩压(51% vs 68%, P = 0.033)。没有腹部肥胖患者达到所有治疗目标,而没有腹部肥胖的患者达到8%。结论:在284例T1D患者中,腹部肥胖与性别、心血管疾病以及心血管危险因素存在显著相关性:低度炎症、收缩压、高HbA1c和甘油三酯。与非肥胖者相比,腹部肥胖患者较少达到HbA1c和收缩压的治疗目标。
Abdominal obesity in type 1 diabetes associated with gender, cardiovascular risk factors and complications, and difficulties achieving treatment targets: a cross sectional study at a secondary care diabetes clinic.
Background: Abdominal obesity is linked to cardiovascular diseases in type 1 diabetes (T1D). The primary aim was to explore associations between abdominal obesity and cardiovascular complications, metabolic and inflammatory factors. The secondary aim was to explore whether achieved recommended treatment targets differed between the obese and non-obese participants.
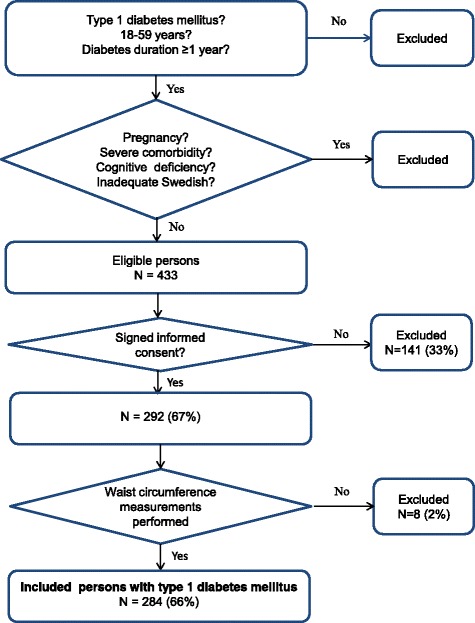
Methods: Cross sectional study of 284 T1D patients (age 18-59 years, men 56%), consecutively recruited from one secondary care specialist diabetes clinic in Sweden. Anthropometrics, blood pressure, serum-lipids and high-sensitivity C-reactive protein (hs-CRP) were collected and supplemented with data from the patients' medical records and from the Swedish National Diabetes Registry. Abdominal obesity was defined as waist circumference men/women (meters): ≥1.02/≥0.88. Hs-CRP was divided into low-, moderate-, and high-risk groups for future cardiovascular events (< 1, 1 to 3, and > 3 to ≤8.9 mg/l). Treatment targets were blood pressure ≤ 130/≤ 80, total cholesterol ≤4.5 mmol/l, LDL: ≤ 2.5 mmol/l, and HbA1c: ≤5 2 mmol/mol (≤ 6.9%). Different explanatory linear, logistic and ordinal regression models were elaborated for the associations, and calibrated and validated for goodness of fit with the data variables.
Results: The prevalence of abdominal obesity was 49/284 (17%), men/women: 8%/29% (P < 0.001). Women (adjusted odds ratio (AOR) 6.5), cardiovascular complications (AOR 5.7), HbA1c > 70 mmol/mol (> 8.6%) (AOR 2.7), systolic blood pressure (per mm Hg) (AOR 1.05), and triglycerides (per mmol/l) (AOR 1.7), were associated with abdominal obesity. Sub analyses (n = 171), showed that abdominal obesity (AOR 5.3) and triglycerides (per mmol/l) (AOR 2.8) were associated with increasing risk levels of hs-CRP. Treatment targets were obtained for fewer patients with abdominal obesity for HbA1c (8% vs 21%, P = 0.044) and systolic blood pressure (51% vs 68%, P = 0.033). No patients with abdominal obesity reached all treatment targets compared to 8% in patients without abdominal obesity.
Conclusions: Significant associations between abdominal obesity and gender, cardiovascular disease, and the cardiovascular risk factors low-grade inflammation, systolic blood pressure, high HbA1c, and triglycerides, were found in 284 T1D patients. Fewer patients with abdominal obesity reached the treatment targets for HbA1c and systolic blood pressure compared to the non-obese.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
