Dennis Röser, Stephanie Bjerrum, Marie Helleberg, Henrik Vedel Nielsen, Kim Peter David, Søren Thybo, Christen Rune Stensvold
{"title":"探险旅游和血吸虫病:一群丹麦学生在乌干达漂流后的血清学和临床发现。","authors":"Dennis Röser, Stephanie Bjerrum, Marie Helleberg, Henrik Vedel Nielsen, Kim Peter David, Søren Thybo, Christen Rune Stensvold","doi":"10.1099/jmmcr.0.005141","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Diagnosis of schistosomiasis in travellers is a clinical challenge, since cases may present with no symptoms or a few non-specific symptoms. Here, we report on the laboratory and clinical findings in Danish travellers exposed to <i>Schistosoma</i>-infested water during white-water rafting on the Ugandan part of the upper Nile River in July 2009.</p><p><strong>Case presentation: </strong>Forty travellers were offered screening for <i>Schistosoma</i>-specific antibodies. Serological tests were performed 6-65 weeks after exposure. A self-reporting questionnaire was used to collect information on travel activity and health history, fresh water exposure, and symptoms. Seropositive cases were referred to hospitals where clinical and biochemical data were collected. <i>Schistosoma</i>-specific antibodies were detected in 13/35 (37 %) exposed participants, with 4/13 (31 %) seroconverting later than 2 months following exposure. Four of thirteen (31 %) cases reported ≥3 symptoms compatible with schistosomiasis, with a mean onset of 41 days following exposure. No <i>Schistosoma</i> eggs were detected in stool or urine in any of the cases. Peripheral eosinophilia (>0.45×10<sup>9</sup> cells l<sup>-1</sup>) was seen in 4/13 cases, while IgE levels were normal in all cases.</p><p><strong>Conclusion: </strong>Schistosomiasis in travellers is not necessarily associated with specific signs or symptoms, eosinophilia, raised IgE levels, or detection of eggs. The only prognostic factor for infection was exposure to freshwater in a <i>Schistosoma</i>-endemic area. Seroconversion may occur later than 2 months after exposure and therefore - in the absence of other diagnostic evidence - serology testing should be performed up to at least 2-3 months following exposure to be able to rule out schistosomiasis.</p>","PeriodicalId":73559,"journal":{"name":"JMM case reports","volume":"5 4","pages":"e005141"},"PeriodicalIF":0.0000,"publicationDate":"2018-02-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5982149/pdf/","citationCount":"8","resultStr":"{\"title\":\"Adventure tourism and schistosomiasis: serology and clinical findings in a group of Danish students after white-water rafting in Uganda.\",\"authors\":\"Dennis Röser, Stephanie Bjerrum, Marie Helleberg, Henrik Vedel Nielsen, Kim Peter David, Søren Thybo, Christen Rune Stensvold\",\"doi\":\"10.1099/jmmcr.0.005141\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Diagnosis of schistosomiasis in travellers is a clinical challenge, since cases may present with no symptoms or a few non-specific symptoms. Here, we report on the laboratory and clinical findings in Danish travellers exposed to <i>Schistosoma</i>-infested water during white-water rafting on the Ugandan part of the upper Nile River in July 2009.</p><p><strong>Case presentation: </strong>Forty travellers were offered screening for <i>Schistosoma</i>-specific antibodies. Serological tests were performed 6-65 weeks after exposure. A self-reporting questionnaire was used to collect information on travel activity and health history, fresh water exposure, and symptoms. Seropositive cases were referred to hospitals where clinical and biochemical data were collected. <i>Schistosoma</i>-specific antibodies were detected in 13/35 (37 %) exposed participants, with 4/13 (31 %) seroconverting later than 2 months following exposure. Four of thirteen (31 %) cases reported ≥3 symptoms compatible with schistosomiasis, with a mean onset of 41 days following exposure. No <i>Schistosoma</i> eggs were detected in stool or urine in any of the cases. Peripheral eosinophilia (>0.45×10<sup>9</sup> cells l<sup>-1</sup>) was seen in 4/13 cases, while IgE levels were normal in all cases.</p><p><strong>Conclusion: </strong>Schistosomiasis in travellers is not necessarily associated with specific signs or symptoms, eosinophilia, raised IgE levels, or detection of eggs. The only prognostic factor for infection was exposure to freshwater in a <i>Schistosoma</i>-endemic area. Seroconversion may occur later than 2 months after exposure and therefore - in the absence of other diagnostic evidence - serology testing should be performed up to at least 2-3 months following exposure to be able to rule out schistosomiasis.</p>\",\"PeriodicalId\":73559,\"journal\":{\"name\":\"JMM case reports\",\"volume\":\"5 4\",\"pages\":\"e005141\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2018-02-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5982149/pdf/\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JMM case reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1099/jmmcr.0.005141\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/4/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMM case reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1099/jmmcr.0.005141","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/4/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Adventure tourism and schistosomiasis: serology and clinical findings in a group of Danish students after white-water rafting in Uganda.
Introduction: Diagnosis of schistosomiasis in travellers is a clinical challenge, since cases may present with no symptoms or a few non-specific symptoms. Here, we report on the laboratory and clinical findings in Danish travellers exposed to Schistosoma-infested water during white-water rafting on the Ugandan part of the upper Nile River in July 2009.
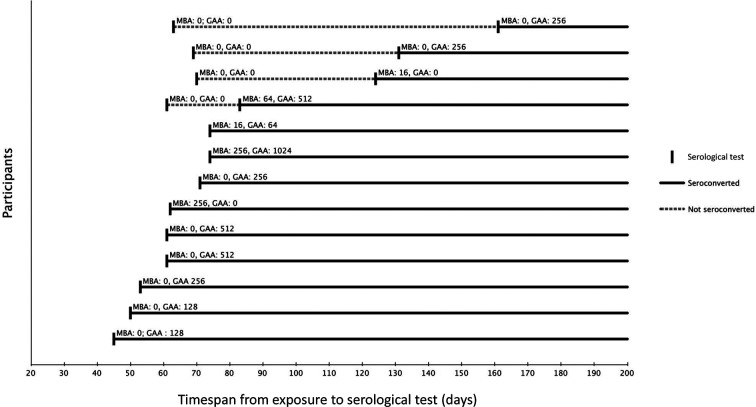
Case presentation: Forty travellers were offered screening for Schistosoma-specific antibodies. Serological tests were performed 6-65 weeks after exposure. A self-reporting questionnaire was used to collect information on travel activity and health history, fresh water exposure, and symptoms. Seropositive cases were referred to hospitals where clinical and biochemical data were collected. Schistosoma-specific antibodies were detected in 13/35 (37 %) exposed participants, with 4/13 (31 %) seroconverting later than 2 months following exposure. Four of thirteen (31 %) cases reported ≥3 symptoms compatible with schistosomiasis, with a mean onset of 41 days following exposure. No Schistosoma eggs were detected in stool or urine in any of the cases. Peripheral eosinophilia (>0.45×109 cells l-1) was seen in 4/13 cases, while IgE levels were normal in all cases.
Conclusion: Schistosomiasis in travellers is not necessarily associated with specific signs or symptoms, eosinophilia, raised IgE levels, or detection of eggs. The only prognostic factor for infection was exposure to freshwater in a Schistosoma-endemic area. Seroconversion may occur later than 2 months after exposure and therefore - in the absence of other diagnostic evidence - serology testing should be performed up to at least 2-3 months following exposure to be able to rule out schistosomiasis.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
