{"title":"被动抬腿手法对成人心脏手术麻醉诱导过程中血流动力学稳定性的影响。","authors":"Solmaz Fakhari, Eissa Bilehjani, Haleh Farzin, Hojjat Pourfathi, Mohsen Chalabianlou","doi":"10.2147/IBPC.S126514","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Some cardiac patients do not tolerate the intravenous fluid load commonly administered before anesthesia induction. This study investigated preinduction passive leg-raising maneuver (PLRM) as an alternative method to fluid loading before cardiac anesthesia.</p><p><strong>Methods and materials: </strong>During a 6-month period, 120 adult elective heart surgery patients were enrolled in this study and allocated into 2 groups: PLRM group vs control group (n=60). Anesthesia was induced using midazolam, fentanyl, and cisatracurium. Initially, 250 mL of fluid was administrated intravenously in all of patients before anesthesia induction. Then in the PLRM group, PLRM was performed starting 2 minutes before anesthesia induction and continued for 20 minutes after tracheal intubation. In the control group, anesthesia was induced in a simple supine position. Heart rate, invasive mean arterial blood pressure (MAP), and central venous pressure (CVP) were recorded before PLRM, before anesthetic induction, before laryngoscopy, and at 5, 10, and 20 minutes after tracheal intubation. The hypotension episode rate (MAP <70 mmHg) and CVP changes were compared between the 2 groups. The predictive value of the ≥3 mmHg increase in CVP value in response to PLRM for hypotension prevention was defined.</p><p><strong>Results: </strong>Hypotension rates were lower in the PLRM group (63.3% vs 81.6%; <i>P</i>-value 0.04), and MAP was higher among PLRM patients immediately before anesthetic injection, before laryngoscopy, and 20 minutes after intubation, compared to the control group. PLRM increased CVP by 3.57±4.9 mmHg (from 7.50±2.94 to 11.05±3.55 mmHg), which required several minutes to reach peak value, returning to baseline after 15 minutes. This change did not correlate to subsequent MAP changes; an increase in the CVP value ≥3 mmHg decreased the postinduction hypotension rate by 62.50%.</p><p><strong>Conclusion: </strong>Preinduction PLRM can provide a more stable hemodynamic status in adult cardiac surgery patients and decreases anesthesia-induced hypotension rates by 62.50%. Rate of the changes in the CVP value caused by PLRM is not predictive of subsequent MAP changes.</p>","PeriodicalId":45299,"journal":{"name":"Integrated Blood Pressure Control","volume":"11 ","pages":"57-63"},"PeriodicalIF":1.5000,"publicationDate":"2018-06-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/IBPC.S126514","citationCount":"4","resultStr":"{\"title\":\"The effect of passive leg-raising maneuver on hemodynamic stability during anesthesia induction for adult cardiac surgery.\",\"authors\":\"Solmaz Fakhari, Eissa Bilehjani, Haleh Farzin, Hojjat Pourfathi, Mohsen Chalabianlou\",\"doi\":\"10.2147/IBPC.S126514\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Some cardiac patients do not tolerate the intravenous fluid load commonly administered before anesthesia induction. This study investigated preinduction passive leg-raising maneuver (PLRM) as an alternative method to fluid loading before cardiac anesthesia.</p><p><strong>Methods and materials: </strong>During a 6-month period, 120 adult elective heart surgery patients were enrolled in this study and allocated into 2 groups: PLRM group vs control group (n=60). Anesthesia was induced using midazolam, fentanyl, and cisatracurium. Initially, 250 mL of fluid was administrated intravenously in all of patients before anesthesia induction. Then in the PLRM group, PLRM was performed starting 2 minutes before anesthesia induction and continued for 20 minutes after tracheal intubation. In the control group, anesthesia was induced in a simple supine position. Heart rate, invasive mean arterial blood pressure (MAP), and central venous pressure (CVP) were recorded before PLRM, before anesthetic induction, before laryngoscopy, and at 5, 10, and 20 minutes after tracheal intubation. The hypotension episode rate (MAP <70 mmHg) and CVP changes were compared between the 2 groups. The predictive value of the ≥3 mmHg increase in CVP value in response to PLRM for hypotension prevention was defined.</p><p><strong>Results: </strong>Hypotension rates were lower in the PLRM group (63.3% vs 81.6%; <i>P</i>-value 0.04), and MAP was higher among PLRM patients immediately before anesthetic injection, before laryngoscopy, and 20 minutes after intubation, compared to the control group. PLRM increased CVP by 3.57±4.9 mmHg (from 7.50±2.94 to 11.05±3.55 mmHg), which required several minutes to reach peak value, returning to baseline after 15 minutes. This change did not correlate to subsequent MAP changes; an increase in the CVP value ≥3 mmHg decreased the postinduction hypotension rate by 62.50%.</p><p><strong>Conclusion: </strong>Preinduction PLRM can provide a more stable hemodynamic status in adult cardiac surgery patients and decreases anesthesia-induced hypotension rates by 62.50%. Rate of the changes in the CVP value caused by PLRM is not predictive of subsequent MAP changes.</p>\",\"PeriodicalId\":45299,\"journal\":{\"name\":\"Integrated Blood Pressure Control\",\"volume\":\"11 \",\"pages\":\"57-63\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2018-06-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.2147/IBPC.S126514\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Integrated Blood Pressure Control\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/IBPC.S126514\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Integrated Blood Pressure Control","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/IBPC.S126514","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 4
摘要
导读:一些心脏病人不能忍受通常在麻醉诱导前给予的静脉液体负荷。本研究探讨了诱导前被动抬腿术(PLRM)作为心脏麻醉前液体负荷的替代方法。方法与材料:在6个月的时间内,120例成人择期心脏手术患者被纳入本研究,分为两组:PLRM组和对照组(n=60)。麻醉采用咪达唑仑、芬太尼和顺阿曲库铵诱导。在麻醉诱导前,所有患者均静脉滴注250 mL液体。PLRM组在麻醉诱导前2分钟开始PLRM,气管插管后持续20分钟。对照组采用单纯仰卧位诱导麻醉。记录PLRM前、麻醉诱导前、喉镜检查前、气管插管后5、10、20分钟的心率、有创平均动脉血压(MAP)、中心静脉压(CVP)。低血压发作率(MAP)结果:PLRM组低血压发生率较低(63.3% vs 81.6%;p值为0.04),且PLRM患者在麻醉注射前、喉镜检查前和插管后20分钟的MAP高于对照组。PLRM使CVP增加3.57±4.9 mmHg(从7.50±2.94增加到11.05±3.55 mmHg),达到峰值需要几分钟,15分钟后恢复到基线。这一变化与随后的MAP变化无关;CVP值≥3 mmHg升高可使诱导后低血压率降低62.50%。结论:诱导前PLRM可为成人心脏手术患者提供更稳定的血流动力学状态,使麻醉所致低血压率降低62.50%。PLRM引起的CVP值的变化率不能预测随后的MAP变化。
The effect of passive leg-raising maneuver on hemodynamic stability during anesthesia induction for adult cardiac surgery.
Introduction: Some cardiac patients do not tolerate the intravenous fluid load commonly administered before anesthesia induction. This study investigated preinduction passive leg-raising maneuver (PLRM) as an alternative method to fluid loading before cardiac anesthesia.
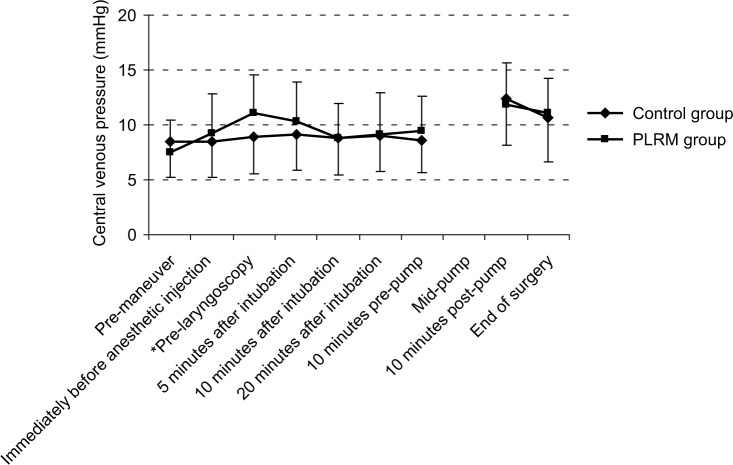
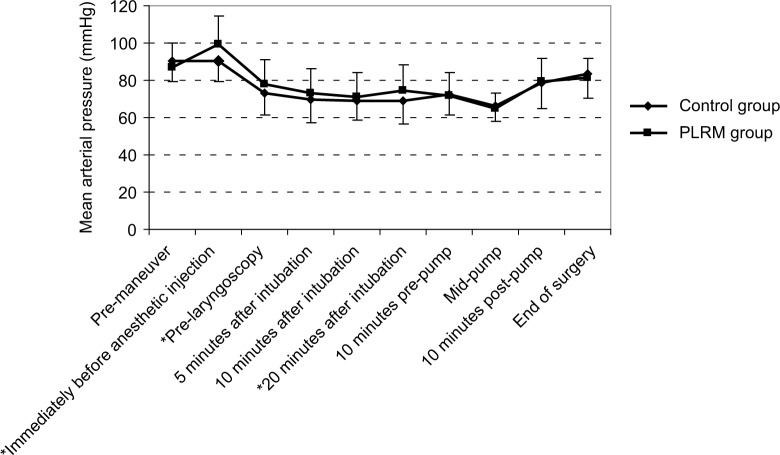
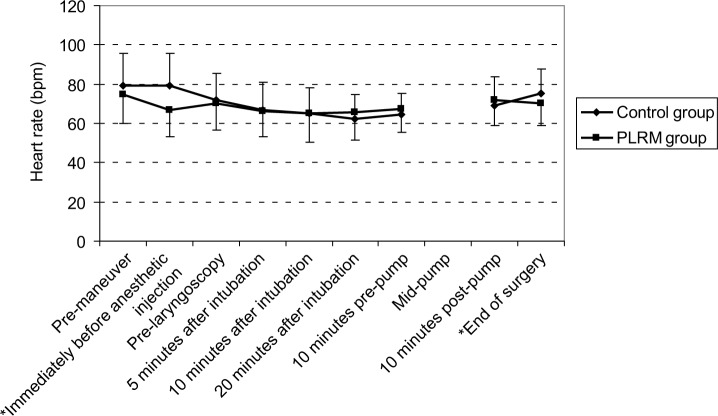
Methods and materials: During a 6-month period, 120 adult elective heart surgery patients were enrolled in this study and allocated into 2 groups: PLRM group vs control group (n=60). Anesthesia was induced using midazolam, fentanyl, and cisatracurium. Initially, 250 mL of fluid was administrated intravenously in all of patients before anesthesia induction. Then in the PLRM group, PLRM was performed starting 2 minutes before anesthesia induction and continued for 20 minutes after tracheal intubation. In the control group, anesthesia was induced in a simple supine position. Heart rate, invasive mean arterial blood pressure (MAP), and central venous pressure (CVP) were recorded before PLRM, before anesthetic induction, before laryngoscopy, and at 5, 10, and 20 minutes after tracheal intubation. The hypotension episode rate (MAP <70 mmHg) and CVP changes were compared between the 2 groups. The predictive value of the ≥3 mmHg increase in CVP value in response to PLRM for hypotension prevention was defined.
Results: Hypotension rates were lower in the PLRM group (63.3% vs 81.6%; P-value 0.04), and MAP was higher among PLRM patients immediately before anesthetic injection, before laryngoscopy, and 20 minutes after intubation, compared to the control group. PLRM increased CVP by 3.57±4.9 mmHg (from 7.50±2.94 to 11.05±3.55 mmHg), which required several minutes to reach peak value, returning to baseline after 15 minutes. This change did not correlate to subsequent MAP changes; an increase in the CVP value ≥3 mmHg decreased the postinduction hypotension rate by 62.50%.
Conclusion: Preinduction PLRM can provide a more stable hemodynamic status in adult cardiac surgery patients and decreases anesthesia-induced hypotension rates by 62.50%. Rate of the changes in the CVP value caused by PLRM is not predictive of subsequent MAP changes.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
