Alexis Llewellyn, Mark Simmonds, Will L Irving, Ginny Brunton, Amanda J Sowden
{"title":"HIV和丙型肝炎合并感染患者的抗逆转录病毒治疗和肝脏疾病进展:一项系统回顾和荟萃分析","authors":"Alexis Llewellyn, Mark Simmonds, Will L Irving, Ginny Brunton, Amanda J Sowden","doi":"10.1186/s41124-016-0015-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>HIV co-infection exacerbates hepatitis C disease, increasing the risk of cirrhosis and hepatitis C-related mortality. Combination antiretroviral therapy (cART) is the current standard treatment for co-infected individuals, but the impact of cART and antiretroviral (ARV) monotherapy on liver disease in this population is unclear. We aimed to assess the effect of cART and ARV monotherapy on liver disease progression and liver-related mortality in individuals co-infected with HIV and chronic hepatitis C.</p><p><strong>Methods: </strong>A systematic review with meta-analyses was conducted. MEDLINE and EMBASE bibliographic databases were searched up to September 2015. Study quality was assessed using a modified Newcastle-Ottawa scale. Results were synthesised narratively and by meta-analysis.</p><p><strong>Results: </strong>Fourteen observational studies were included. In analyses that adjusted for potential confounders, risk of liver-related mortality was significantly lower in patients receiving cART (hazard ratio/odds ratio 0.31, 95 % CI 0.14 to 0.70). Results were similar in unadjusted analyses (relative risk 0.40, 95 % CI 0.29 to 0.55). For outcomes where meta-analysis could not be performed, results were less consistent. Some studies found cART was associated with lower incidence of, or slower progression of liver disease, fibrosis and cirrhosis, while others showed no evidence of benefit. We found no evidence of liver-related harm from cART or ARV monotherapy compared with no HIV therapy.</p><p><strong>Conclusions: </strong>cART was associated with significantly lower liver-related mortality in patients co-infected with HIV and HCV. Evidence of a positive association between cART and/or ARV monotherapy and liver-disease progression was less clear, but there was no evidence to suggest that the absence of antiretroviral therapy was preferable.</p>","PeriodicalId":91692,"journal":{"name":"Hepatology, medicine and policy","volume":"1 ","pages":"10"},"PeriodicalIF":0.0000,"publicationDate":"2016-08-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s41124-016-0015-7","citationCount":"4","resultStr":"{\"title\":\"Antiretroviral therapy and liver disease progression in HIV and hepatitis C co-infected patients: a systematic review and meta-analysis.\",\"authors\":\"Alexis Llewellyn, Mark Simmonds, Will L Irving, Ginny Brunton, Amanda J Sowden\",\"doi\":\"10.1186/s41124-016-0015-7\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>HIV co-infection exacerbates hepatitis C disease, increasing the risk of cirrhosis and hepatitis C-related mortality. Combination antiretroviral therapy (cART) is the current standard treatment for co-infected individuals, but the impact of cART and antiretroviral (ARV) monotherapy on liver disease in this population is unclear. We aimed to assess the effect of cART and ARV monotherapy on liver disease progression and liver-related mortality in individuals co-infected with HIV and chronic hepatitis C.</p><p><strong>Methods: </strong>A systematic review with meta-analyses was conducted. MEDLINE and EMBASE bibliographic databases were searched up to September 2015. Study quality was assessed using a modified Newcastle-Ottawa scale. Results were synthesised narratively and by meta-analysis.</p><p><strong>Results: </strong>Fourteen observational studies were included. In analyses that adjusted for potential confounders, risk of liver-related mortality was significantly lower in patients receiving cART (hazard ratio/odds ratio 0.31, 95 % CI 0.14 to 0.70). Results were similar in unadjusted analyses (relative risk 0.40, 95 % CI 0.29 to 0.55). For outcomes where meta-analysis could not be performed, results were less consistent. Some studies found cART was associated with lower incidence of, or slower progression of liver disease, fibrosis and cirrhosis, while others showed no evidence of benefit. We found no evidence of liver-related harm from cART or ARV monotherapy compared with no HIV therapy.</p><p><strong>Conclusions: </strong>cART was associated with significantly lower liver-related mortality in patients co-infected with HIV and HCV. Evidence of a positive association between cART and/or ARV monotherapy and liver-disease progression was less clear, but there was no evidence to suggest that the absence of antiretroviral therapy was preferable.</p>\",\"PeriodicalId\":91692,\"journal\":{\"name\":\"Hepatology, medicine and policy\",\"volume\":\"1 \",\"pages\":\"10\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2016-08-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s41124-016-0015-7\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Hepatology, medicine and policy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41124-016-0015-7\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2016/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Hepatology, medicine and policy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41124-016-0015-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 4
摘要
背景:HIV合并感染加重了丙型肝炎疾病,增加了肝硬化和丙型肝炎相关死亡率的风险。抗逆转录病毒联合治疗(cART)是目前合并感染个体的标准治疗方法,但cART和抗逆转录病毒(ARV)单药治疗对这类人群肝病的影响尚不清楚。我们的目的是评估cART和ARV单药治疗对合并HIV和慢性丙型肝炎患者肝病进展和肝脏相关死亡率的影响。方法:进行了一项系统综述和荟萃分析。检索截至2015年9月的MEDLINE和EMBASE书目数据库。采用改良的纽卡斯尔-渥太华量表评估研究质量。结果通过叙述和荟萃分析进行综合。结果:纳入14项观察性研究。在对潜在混杂因素进行校正的分析中,接受cART的患者肝脏相关死亡风险显著降低(风险比/优势比0.31,95% CI 0.14至0.70)。未调整分析的结果相似(相对危险度0.40,95% CI 0.29 ~ 0.55)。对于不能进行荟萃分析的结果,结果不太一致。一些研究发现,cART与肝脏疾病、纤维化和肝硬化的发病率较低或进展较慢有关,而其他研究则没有显示出益处的证据。与未接受HIV治疗相比,我们没有发现cART或ARV单药治疗有肝脏相关损害的证据。结论:cART与HIV和HCV合并感染患者的肝脏相关死亡率显著降低相关。cART和/或ARV单药治疗与肝病进展之间正相关的证据尚不清楚,但没有证据表明不使用抗逆转录病毒治疗更好。
Antiretroviral therapy and liver disease progression in HIV and hepatitis C co-infected patients: a systematic review and meta-analysis.
Background: HIV co-infection exacerbates hepatitis C disease, increasing the risk of cirrhosis and hepatitis C-related mortality. Combination antiretroviral therapy (cART) is the current standard treatment for co-infected individuals, but the impact of cART and antiretroviral (ARV) monotherapy on liver disease in this population is unclear. We aimed to assess the effect of cART and ARV monotherapy on liver disease progression and liver-related mortality in individuals co-infected with HIV and chronic hepatitis C.
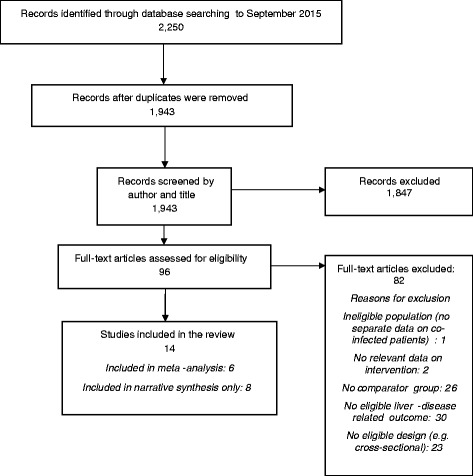
Methods: A systematic review with meta-analyses was conducted. MEDLINE and EMBASE bibliographic databases were searched up to September 2015. Study quality was assessed using a modified Newcastle-Ottawa scale. Results were synthesised narratively and by meta-analysis.
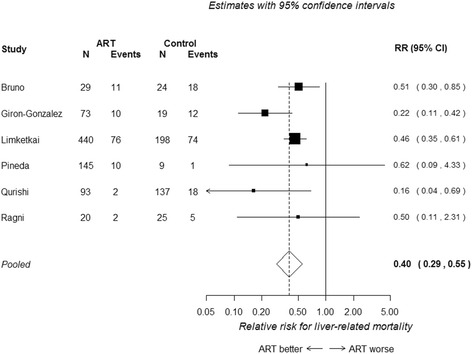
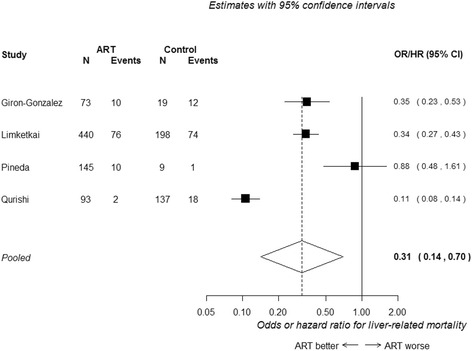
Results: Fourteen observational studies were included. In analyses that adjusted for potential confounders, risk of liver-related mortality was significantly lower in patients receiving cART (hazard ratio/odds ratio 0.31, 95 % CI 0.14 to 0.70). Results were similar in unadjusted analyses (relative risk 0.40, 95 % CI 0.29 to 0.55). For outcomes where meta-analysis could not be performed, results were less consistent. Some studies found cART was associated with lower incidence of, or slower progression of liver disease, fibrosis and cirrhosis, while others showed no evidence of benefit. We found no evidence of liver-related harm from cART or ARV monotherapy compared with no HIV therapy.
Conclusions: cART was associated with significantly lower liver-related mortality in patients co-infected with HIV and HCV. Evidence of a positive association between cART and/or ARV monotherapy and liver-disease progression was less clear, but there was no evidence to suggest that the absence of antiretroviral therapy was preferable.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
