Jennifer Blythe, Eva Herrmann, Dominik Faust, Stephan Falk, Tina Edwards-Lehr, Florian Stockhausen, Ernst Hanisch, Alexander Buia
{"title":"急性胆囊炎——现实世界临床环境中的队列研究(REWO研究,NCT02796443)。","authors":"Jennifer Blythe, Eva Herrmann, Dominik Faust, Stephan Falk, Tina Edwards-Lehr, Florian Stockhausen, Ernst Hanisch, Alexander Buia","doi":"10.2147/POR.S169255","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>For decades, the optimal timing of surgery for acute cholecystitis has been controversial. Recent meta-analyses and population-based studies favor early surgery. One recent large randomized trial has demonstrated that a delayed approach increases morbidity and cost compared to early surgery within 24 hours of hospital admission. Since cases of severe cholecystitis were excluded from this trial, we argue that these results do not reflect real-world clinical situations. From our point of view, these results were in contrast to the clinical experience with our patients; so, we decided to analyze critically all our patients with the null hypothesis that the patients treated with a delayed cholecystectomy after an acute cholecystitis have a similar or even better outcome than those treated with an early operative approach.</p><p><strong>Patients and methods: </strong>We retrospectively analyzed clinical data from all patients with cholecystectomies in the period between January 2006 and September 2015. A total of 1,723 patients were categorized into four groups: early (n=138): urgent surgery of patients with acute cholecystitis within the first 72 hours of the onset of symptoms; intermediate (n=297): surgery of patients with acute cholecystitis within an average of 10 days after the onset of symptoms; delayed (n=427): initial non-surgical treatment of acute cholecystitis with surgery performed within 6-12 weeks of the onset of symptoms; and elective (n=868): cholecystectomy within a symptom-free interval of choice in patients with symptomatic cholecystolithiasis without signs of acute cholecystitis.</p><p><strong>Results: </strong>In a real-world scenario, early/intermediate cholecystectomy in acute cholecystitis was associated with a significant increase in morbidity and mortality (Clavien-Dindo score) compared to a delayed approach with surgery performed 6-12 weeks after the onset of symptoms. The adjusted linear rank statistics showed a decrease in the complication score with values of 2.29 in the early group, 0.48 in the intermediate group, -0.26 in the delayed group and -2.12 in the elective group. The results translate into a continuous decrease of the complication score from early over intermediate and delayed to the elective group.</p><p><strong>Conclusion: </strong>These results demonstrate that delayed cholecystectomy can be performed safely. In cases with severe cholecystitis, early and/or intermediate approaches still have a relatively high risk of morbidity and mortality.</p>","PeriodicalId":20399,"journal":{"name":"Pragmatic and Observational Research","volume":"9 ","pages":"69-75"},"PeriodicalIF":2.7000,"publicationDate":"2018-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/POR.S169255","citationCount":"13","resultStr":"{\"title\":\"Acute cholecystitis - a cohort study in a real-world clinical setting (REWO study, NCT02796443).\",\"authors\":\"Jennifer Blythe, Eva Herrmann, Dominik Faust, Stephan Falk, Tina Edwards-Lehr, Florian Stockhausen, Ernst Hanisch, Alexander Buia\",\"doi\":\"10.2147/POR.S169255\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>For decades, the optimal timing of surgery for acute cholecystitis has been controversial. Recent meta-analyses and population-based studies favor early surgery. One recent large randomized trial has demonstrated that a delayed approach increases morbidity and cost compared to early surgery within 24 hours of hospital admission. Since cases of severe cholecystitis were excluded from this trial, we argue that these results do not reflect real-world clinical situations. From our point of view, these results were in contrast to the clinical experience with our patients; so, we decided to analyze critically all our patients with the null hypothesis that the patients treated with a delayed cholecystectomy after an acute cholecystitis have a similar or even better outcome than those treated with an early operative approach.</p><p><strong>Patients and methods: </strong>We retrospectively analyzed clinical data from all patients with cholecystectomies in the period between January 2006 and September 2015. A total of 1,723 patients were categorized into four groups: early (n=138): urgent surgery of patients with acute cholecystitis within the first 72 hours of the onset of symptoms; intermediate (n=297): surgery of patients with acute cholecystitis within an average of 10 days after the onset of symptoms; delayed (n=427): initial non-surgical treatment of acute cholecystitis with surgery performed within 6-12 weeks of the onset of symptoms; and elective (n=868): cholecystectomy within a symptom-free interval of choice in patients with symptomatic cholecystolithiasis without signs of acute cholecystitis.</p><p><strong>Results: </strong>In a real-world scenario, early/intermediate cholecystectomy in acute cholecystitis was associated with a significant increase in morbidity and mortality (Clavien-Dindo score) compared to a delayed approach with surgery performed 6-12 weeks after the onset of symptoms. The adjusted linear rank statistics showed a decrease in the complication score with values of 2.29 in the early group, 0.48 in the intermediate group, -0.26 in the delayed group and -2.12 in the elective group. The results translate into a continuous decrease of the complication score from early over intermediate and delayed to the elective group.</p><p><strong>Conclusion: </strong>These results demonstrate that delayed cholecystectomy can be performed safely. In cases with severe cholecystitis, early and/or intermediate approaches still have a relatively high risk of morbidity and mortality.</p>\",\"PeriodicalId\":20399,\"journal\":{\"name\":\"Pragmatic and Observational Research\",\"volume\":\"9 \",\"pages\":\"69-75\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2018-10-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.2147/POR.S169255\",\"citationCount\":\"13\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pragmatic and Observational Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/POR.S169255\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pragmatic and Observational Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/POR.S169255","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Acute cholecystitis - a cohort study in a real-world clinical setting (REWO study, NCT02796443).
Background: For decades, the optimal timing of surgery for acute cholecystitis has been controversial. Recent meta-analyses and population-based studies favor early surgery. One recent large randomized trial has demonstrated that a delayed approach increases morbidity and cost compared to early surgery within 24 hours of hospital admission. Since cases of severe cholecystitis were excluded from this trial, we argue that these results do not reflect real-world clinical situations. From our point of view, these results were in contrast to the clinical experience with our patients; so, we decided to analyze critically all our patients with the null hypothesis that the patients treated with a delayed cholecystectomy after an acute cholecystitis have a similar or even better outcome than those treated with an early operative approach.
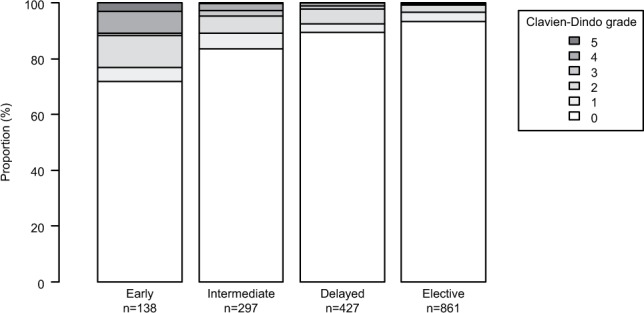
Patients and methods: We retrospectively analyzed clinical data from all patients with cholecystectomies in the period between January 2006 and September 2015. A total of 1,723 patients were categorized into four groups: early (n=138): urgent surgery of patients with acute cholecystitis within the first 72 hours of the onset of symptoms; intermediate (n=297): surgery of patients with acute cholecystitis within an average of 10 days after the onset of symptoms; delayed (n=427): initial non-surgical treatment of acute cholecystitis with surgery performed within 6-12 weeks of the onset of symptoms; and elective (n=868): cholecystectomy within a symptom-free interval of choice in patients with symptomatic cholecystolithiasis without signs of acute cholecystitis.
Results: In a real-world scenario, early/intermediate cholecystectomy in acute cholecystitis was associated with a significant increase in morbidity and mortality (Clavien-Dindo score) compared to a delayed approach with surgery performed 6-12 weeks after the onset of symptoms. The adjusted linear rank statistics showed a decrease in the complication score with values of 2.29 in the early group, 0.48 in the intermediate group, -0.26 in the delayed group and -2.12 in the elective group. The results translate into a continuous decrease of the complication score from early over intermediate and delayed to the elective group.
Conclusion: These results demonstrate that delayed cholecystectomy can be performed safely. In cases with severe cholecystitis, early and/or intermediate approaches still have a relatively high risk of morbidity and mortality.
期刊介绍:
Pragmatic and Observational Research is an international, peer-reviewed, open-access journal that publishes data from studies designed to closely reflect medical interventions in real-world clinical practice, providing insights beyond classical randomized controlled trials (RCTs). While RCTs maximize internal validity for cause-and-effect relationships, they often represent only specific patient groups. This journal aims to complement such studies by providing data that better mirrors real-world patients and the usage of medicines, thus informing guidelines and enhancing the applicability of research findings across diverse patient populations encountered in everyday clinical practice.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
