Laurence Gariépy-Assal, Rodney D Gilbert, Aleksas Žiaugra, Bethany Joy Foster
{"title":"Denys-Drash综合征的管理:基于国际调查的病例系列。","authors":"Laurence Gariépy-Assal, Rodney D Gilbert, Aleksas Žiaugra, Bethany Joy Foster","doi":"10.5414/CNCS109515","DOIUrl":null,"url":null,"abstract":"<p><p>Denys-Drash syndrome (DDS), a condition caused by mutations in the tumor-suppressor gene WT-1, is associated with a triad of disorders: ambiguous genitalia, nephrotic syndrome leading to end-stage renal disease (ESRD), and Wilms' tumor. Given the variable disease course, management is challenging. We aimed to describe the evolution of DDS and the range of management strategies by summarizing the clinical courses of cases collected from a questionnaire sent to the international pediatric nephrology community. 15 respondents provided information on 23 patients; 21 DDS cases were confirmed and analyzed. At DDS diagnosis, 6 patients had a Wilms' tumor (group A) and 15 had no Wilms' tumor (group B). Three group A patients had unilateral nephrectomy. Two of these still had renal function, with no second tumor, at 36 months and 16 years of age, and 1 progressed to ESRD. Three had bilateral nephrectomy before ESRD. Eight group B patients progressed to ESRD, all of whom later had all renal tissue removed. Two group B patients subsequently developed a unilateral Wilms' tumor and had bilateral nephrectomy pre-ESRD. Three had bilateral nephrectomy prior to reaching ESRD without ever having a Wilms' tumor. Two group B patients remained tumor-free with renal function at last follow-up. Two main management approaches were taken: pre-emptive nephrectomy prior to ESRD and conservative surveillance. Based on the known risks associated with ESRD in infants and young children, the variable course of DDS, and the relatively good prognosis associated with Wilms' tumor, a guiding principle of preservation of renal function is most logical. Most would advocate bilateral prophylactic nephrectomy after ESRD is reached due to the high tumor risk, which is likely heightened after transplant.</p>","PeriodicalId":10398,"journal":{"name":"Clinical Nephrology. Case Studies","volume":"6 ","pages":"36-44"},"PeriodicalIF":0.0000,"publicationDate":"2018-11-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6236398/pdf/","citationCount":"9","resultStr":"{\"title\":\"Management of Denys-Drash syndrome: A case series based on an international survey.\",\"authors\":\"Laurence Gariépy-Assal, Rodney D Gilbert, Aleksas Žiaugra, Bethany Joy Foster\",\"doi\":\"10.5414/CNCS109515\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Denys-Drash syndrome (DDS), a condition caused by mutations in the tumor-suppressor gene WT-1, is associated with a triad of disorders: ambiguous genitalia, nephrotic syndrome leading to end-stage renal disease (ESRD), and Wilms' tumor. Given the variable disease course, management is challenging. We aimed to describe the evolution of DDS and the range of management strategies by summarizing the clinical courses of cases collected from a questionnaire sent to the international pediatric nephrology community. 15 respondents provided information on 23 patients; 21 DDS cases were confirmed and analyzed. At DDS diagnosis, 6 patients had a Wilms' tumor (group A) and 15 had no Wilms' tumor (group B). Three group A patients had unilateral nephrectomy. Two of these still had renal function, with no second tumor, at 36 months and 16 years of age, and 1 progressed to ESRD. Three had bilateral nephrectomy before ESRD. Eight group B patients progressed to ESRD, all of whom later had all renal tissue removed. Two group B patients subsequently developed a unilateral Wilms' tumor and had bilateral nephrectomy pre-ESRD. Three had bilateral nephrectomy prior to reaching ESRD without ever having a Wilms' tumor. Two group B patients remained tumor-free with renal function at last follow-up. Two main management approaches were taken: pre-emptive nephrectomy prior to ESRD and conservative surveillance. Based on the known risks associated with ESRD in infants and young children, the variable course of DDS, and the relatively good prognosis associated with Wilms' tumor, a guiding principle of preservation of renal function is most logical. Most would advocate bilateral prophylactic nephrectomy after ESRD is reached due to the high tumor risk, which is likely heightened after transplant.</p>\",\"PeriodicalId\":10398,\"journal\":{\"name\":\"Clinical Nephrology. Case Studies\",\"volume\":\"6 \",\"pages\":\"36-44\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2018-11-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6236398/pdf/\",\"citationCount\":\"9\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Nephrology. Case Studies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5414/CNCS109515\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nephrology. Case Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS109515","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Management of Denys-Drash syndrome: A case series based on an international survey.
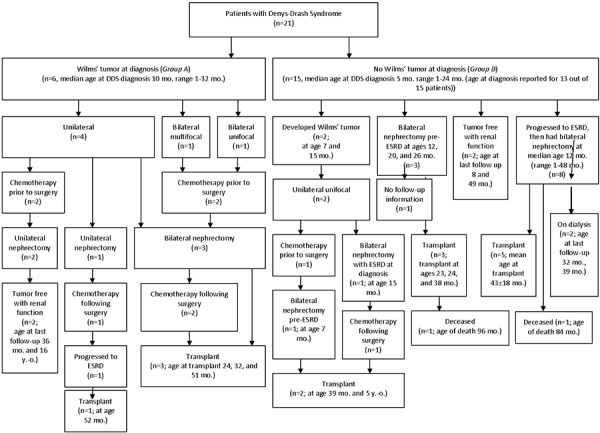
Denys-Drash syndrome (DDS), a condition caused by mutations in the tumor-suppressor gene WT-1, is associated with a triad of disorders: ambiguous genitalia, nephrotic syndrome leading to end-stage renal disease (ESRD), and Wilms' tumor. Given the variable disease course, management is challenging. We aimed to describe the evolution of DDS and the range of management strategies by summarizing the clinical courses of cases collected from a questionnaire sent to the international pediatric nephrology community. 15 respondents provided information on 23 patients; 21 DDS cases were confirmed and analyzed. At DDS diagnosis, 6 patients had a Wilms' tumor (group A) and 15 had no Wilms' tumor (group B). Three group A patients had unilateral nephrectomy. Two of these still had renal function, with no second tumor, at 36 months and 16 years of age, and 1 progressed to ESRD. Three had bilateral nephrectomy before ESRD. Eight group B patients progressed to ESRD, all of whom later had all renal tissue removed. Two group B patients subsequently developed a unilateral Wilms' tumor and had bilateral nephrectomy pre-ESRD. Three had bilateral nephrectomy prior to reaching ESRD without ever having a Wilms' tumor. Two group B patients remained tumor-free with renal function at last follow-up. Two main management approaches were taken: pre-emptive nephrectomy prior to ESRD and conservative surveillance. Based on the known risks associated with ESRD in infants and young children, the variable course of DDS, and the relatively good prognosis associated with Wilms' tumor, a guiding principle of preservation of renal function is most logical. Most would advocate bilateral prophylactic nephrectomy after ESRD is reached due to the high tumor risk, which is likely heightened after transplant.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
