{"title":"脑卒中康复的分层:功能结果的五年概况。","authors":"Bryan Ping Ho Chung","doi":"10.1142/S1013702518500129","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Stroke rehabilitation in inpatient setting requires high intensity of manpower and resources. Early stratification of patients with stroke could facilitate early discharge plan and reduce avoidable length of stay (LOS) in hospital. Stratification of patients with stroke in clinical setting is usually based on functional scores which are quite time-consuming and require a special training to complete the full score.</p><p><strong>Objective: </strong>The objective of the study was to explore whether Modified Functional Ambulation Category (MFAC) can serve as a stratification tool of patients with stroke in inpatient rehabilitation.</p><p><strong>Methods: </strong>This was a retrospective, descriptive study of the demographic, functional outcomes of patients with stroke in an inpatient rehabilitation center. A total of 2,722 patients completed a stroke rehabilitation program from 2011 to 2015 were recruited. The patients were divided into seven groups according to their admission MFAC. The between-group difference in LOS, functional outcomes at admission and discharge including Modified Rivermead Mobility Index (MRMI) and Modified Barthel Index (MBI) as well as MRMI gain, MRMI efficiency, MBI gain, and MBI efficiency were analyzed.</p><p><strong>Results: </strong>Subjects with admission categories of MFAC 2 and 3 had a highly significant ( <math><mi>p</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>001</mn></math> ) MRMI gain (6.2 and 6.6, respectively) and subjects with admission categories of MFAC 3 to 5 had highly significant ( <math><mi>P</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>001</mn></math> ) MRMI efficiency (0.34, 0.40, and 0.39, respectively). The subjects with admission categories of MFAC 2 to 5 had a highly significant ( <math><mi>p</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>001</mn></math> ) MBI gain (9.7, 10.2, 9.3, and 7.0, respectively) and the subjects with admission categories of MFAC 4 to 5 had a highly significant ( <math><mi>p</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>001</mn></math> ) MBI efficiency (0.70 and 0.72, respectively). The subjects with admission categories of MFAC 1 and 2 had a highly significant ( <math><mi>p</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>001</mn></math> ) LOS (27.7 and 26.6, respectively). MFAC profile was also established to represent the distribution of discharge MFAC of subjects according to their admission MFAC. The chance of subjects with admission categories of MFAC 1 and MFAC 2 progress to any kind of walker (MFAC <math><mo>></mo></math> 2) is 12.7% and 58.2%, respectively. The chance of subjects with admission MFAC 3, MFAC 4 and MFAC 5 progress to independent walker (MFAC <math><mo>></mo></math> 5) is 6.7%, 14.8%, and 50.3%, respectively. Both admission MFAC and admission MBI had strong correlations with discharge MFAC ( <math><mi>r</mi> <mo>=</mo> <mn>0</mn> <mo>.</mo> <mn>84</mn></math> , <math><mi>P</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>0001</mn></math> and <math><mi>r</mi> <mo>=</mo> <mn>0</mn> <mo>.</mo> <mn>78</mn></math> , <math><mi>P</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>0001</mn></math> , respectively), discharge MRMI ( <math><mi>r</mi> <mo>=</mo> <mn>0</mn> <mo>.</mo> <mn>82</mn></math> , <math><mi>P</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>0001</mn></math> and <math><mi>r</mi> <mo>=</mo> <mn>0</mn> <mo>.</mo> <mn>78</mn></math> , <math><mi>P</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>0001</mn></math> , respectively) and discharge MBI ( <math><mi>r</mi> <mo>=</mo> <mn>0</mn> <mo>.</mo> <mn>78</mn></math> , <math><mi>P</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>0001</mn></math> and <math><mi>r</mi> <mo>=</mo> <mn>0</mn> <mo>.</mo> <mn>94</mn></math> , <math><mi>P</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>0001</mn></math> , respectively).</p><p><strong>Conclusion: </strong>This study showed that patients on admission with moderate disability in term of MFAC had the greatest mobility gain and basic activities of daily living (ADL) gain from inpatient stroke rehabilitation. Admission MFAC could be a stratification tool of patients with stroke in inpatient rehabilitation.</p>","PeriodicalId":73250,"journal":{"name":"","volume":"38 2","pages":"141-147"},"PeriodicalIF":0.0,"publicationDate":"2018-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1142/S1013702518500129","citationCount":"3","resultStr":"{\"title\":\"Stratification of stroke rehabilitation: Five-year profiles of functional outcomes.\",\"authors\":\"Bryan Ping Ho Chung\",\"doi\":\"10.1142/S1013702518500129\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Stroke rehabilitation in inpatient setting requires high intensity of manpower and resources. Early stratification of patients with stroke could facilitate early discharge plan and reduce avoidable length of stay (LOS) in hospital. Stratification of patients with stroke in clinical setting is usually based on functional scores which are quite time-consuming and require a special training to complete the full score.</p><p><strong>Objective: </strong>The objective of the study was to explore whether Modified Functional Ambulation Category (MFAC) can serve as a stratification tool of patients with stroke in inpatient rehabilitation.</p><p><strong>Methods: </strong>This was a retrospective, descriptive study of the demographic, functional outcomes of patients with stroke in an inpatient rehabilitation center. A total of 2,722 patients completed a stroke rehabilitation program from 2011 to 2015 were recruited. The patients were divided into seven groups according to their admission MFAC. The between-group difference in LOS, functional outcomes at admission and discharge including Modified Rivermead Mobility Index (MRMI) and Modified Barthel Index (MBI) as well as MRMI gain, MRMI efficiency, MBI gain, and MBI efficiency were analyzed.</p><p><strong>Results: </strong>Subjects with admission categories of MFAC 2 and 3 had a highly significant ( <math><mi>p</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>001</mn></math> ) MRMI gain (6.2 and 6.6, respectively) and subjects with admission categories of MFAC 3 to 5 had highly significant ( <math><mi>P</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>001</mn></math> ) MRMI efficiency (0.34, 0.40, and 0.39, respectively). The subjects with admission categories of MFAC 2 to 5 had a highly significant ( <math><mi>p</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>001</mn></math> ) MBI gain (9.7, 10.2, 9.3, and 7.0, respectively) and the subjects with admission categories of MFAC 4 to 5 had a highly significant ( <math><mi>p</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>001</mn></math> ) MBI efficiency (0.70 and 0.72, respectively). The subjects with admission categories of MFAC 1 and 2 had a highly significant ( <math><mi>p</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>001</mn></math> ) LOS (27.7 and 26.6, respectively). MFAC profile was also established to represent the distribution of discharge MFAC of subjects according to their admission MFAC. The chance of subjects with admission categories of MFAC 1 and MFAC 2 progress to any kind of walker (MFAC <math><mo>></mo></math> 2) is 12.7% and 58.2%, respectively. The chance of subjects with admission MFAC 3, MFAC 4 and MFAC 5 progress to independent walker (MFAC <math><mo>></mo></math> 5) is 6.7%, 14.8%, and 50.3%, respectively. Both admission MFAC and admission MBI had strong correlations with discharge MFAC ( <math><mi>r</mi> <mo>=</mo> <mn>0</mn> <mo>.</mo> <mn>84</mn></math> , <math><mi>P</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>0001</mn></math> and <math><mi>r</mi> <mo>=</mo> <mn>0</mn> <mo>.</mo> <mn>78</mn></math> , <math><mi>P</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>0001</mn></math> , respectively), discharge MRMI ( <math><mi>r</mi> <mo>=</mo> <mn>0</mn> <mo>.</mo> <mn>82</mn></math> , <math><mi>P</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>0001</mn></math> and <math><mi>r</mi> <mo>=</mo> <mn>0</mn> <mo>.</mo> <mn>78</mn></math> , <math><mi>P</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>0001</mn></math> , respectively) and discharge MBI ( <math><mi>r</mi> <mo>=</mo> <mn>0</mn> <mo>.</mo> <mn>78</mn></math> , <math><mi>P</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>0001</mn></math> and <math><mi>r</mi> <mo>=</mo> <mn>0</mn> <mo>.</mo> <mn>94</mn></math> , <math><mi>P</mi> <mo><</mo> <mn>0</mn> <mo>.</mo> <mn>0001</mn></math> , respectively).</p><p><strong>Conclusion: </strong>This study showed that patients on admission with moderate disability in term of MFAC had the greatest mobility gain and basic activities of daily living (ADL) gain from inpatient stroke rehabilitation. Admission MFAC could be a stratification tool of patients with stroke in inpatient rehabilitation.</p>\",\"PeriodicalId\":73250,\"journal\":{\"name\":\"\",\"volume\":\"38 2\",\"pages\":\"141-147\"},\"PeriodicalIF\":0.0,\"publicationDate\":\"2018-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1142/S1013702518500129\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1142/S1013702518500129\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2018/8/14 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1142/S1013702518500129","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/8/14 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Stratification of stroke rehabilitation: Five-year profiles of functional outcomes.
Background: Stroke rehabilitation in inpatient setting requires high intensity of manpower and resources. Early stratification of patients with stroke could facilitate early discharge plan and reduce avoidable length of stay (LOS) in hospital. Stratification of patients with stroke in clinical setting is usually based on functional scores which are quite time-consuming and require a special training to complete the full score.
Objective: The objective of the study was to explore whether Modified Functional Ambulation Category (MFAC) can serve as a stratification tool of patients with stroke in inpatient rehabilitation.
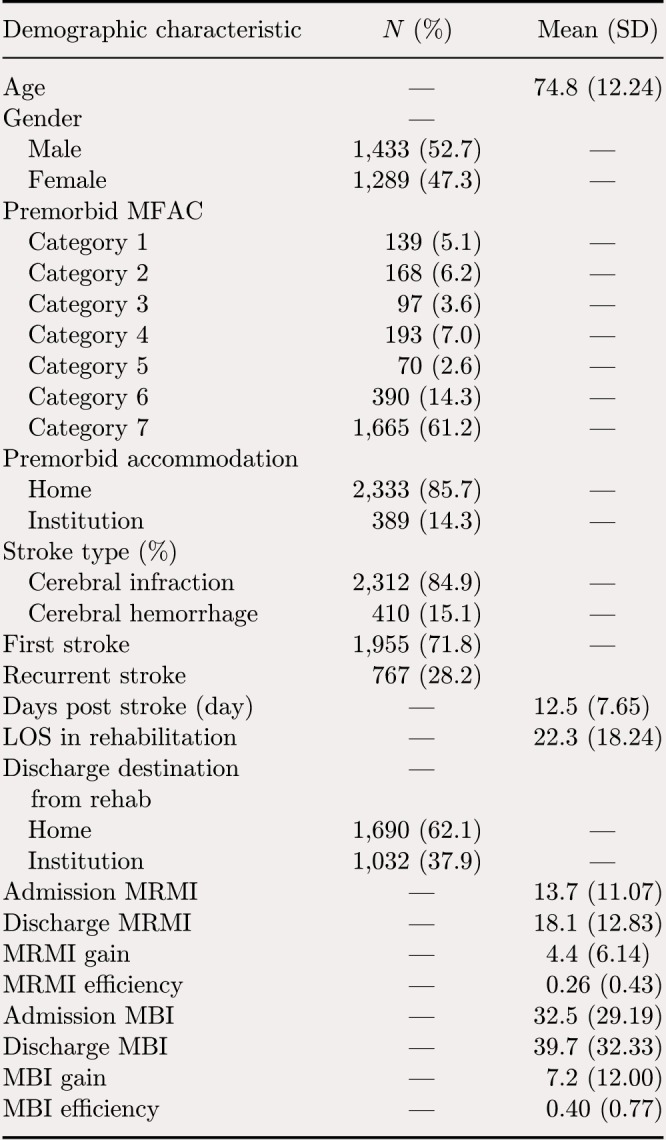
Methods: This was a retrospective, descriptive study of the demographic, functional outcomes of patients with stroke in an inpatient rehabilitation center. A total of 2,722 patients completed a stroke rehabilitation program from 2011 to 2015 were recruited. The patients were divided into seven groups according to their admission MFAC. The between-group difference in LOS, functional outcomes at admission and discharge including Modified Rivermead Mobility Index (MRMI) and Modified Barthel Index (MBI) as well as MRMI gain, MRMI efficiency, MBI gain, and MBI efficiency were analyzed.
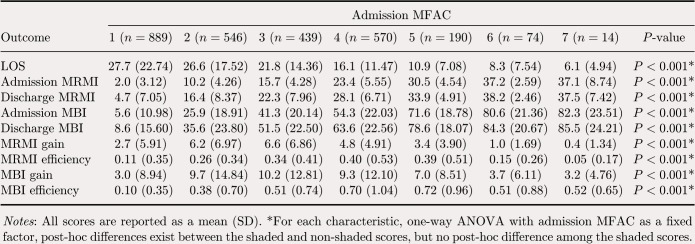
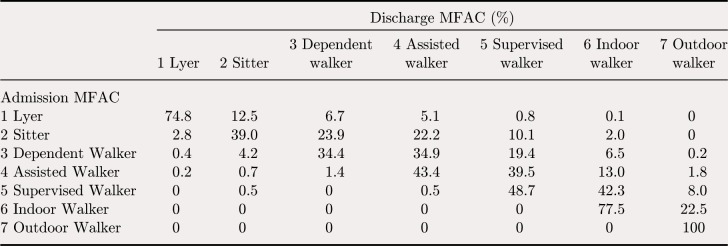
Results: Subjects with admission categories of MFAC 2 and 3 had a highly significant ( ) MRMI gain (6.2 and 6.6, respectively) and subjects with admission categories of MFAC 3 to 5 had highly significant ( ) MRMI efficiency (0.34, 0.40, and 0.39, respectively). The subjects with admission categories of MFAC 2 to 5 had a highly significant ( ) MBI gain (9.7, 10.2, 9.3, and 7.0, respectively) and the subjects with admission categories of MFAC 4 to 5 had a highly significant ( ) MBI efficiency (0.70 and 0.72, respectively). The subjects with admission categories of MFAC 1 and 2 had a highly significant ( ) LOS (27.7 and 26.6, respectively). MFAC profile was also established to represent the distribution of discharge MFAC of subjects according to their admission MFAC. The chance of subjects with admission categories of MFAC 1 and MFAC 2 progress to any kind of walker (MFAC 2) is 12.7% and 58.2%, respectively. The chance of subjects with admission MFAC 3, MFAC 4 and MFAC 5 progress to independent walker (MFAC 5) is 6.7%, 14.8%, and 50.3%, respectively. Both admission MFAC and admission MBI had strong correlations with discharge MFAC ( , and , , respectively), discharge MRMI ( , and , , respectively) and discharge MBI ( , and , , respectively).
Conclusion: This study showed that patients on admission with moderate disability in term of MFAC had the greatest mobility gain and basic activities of daily living (ADL) gain from inpatient stroke rehabilitation. Admission MFAC could be a stratification tool of patients with stroke in inpatient rehabilitation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
