Philip F Lavere, Nikunj A Rana, Michael P Kinsky, J Sean Funston, Sharif S Mohamed, Mohamad R Chaaban
{"title":"艾司洛尔与拉贝他洛尔在内镜鼻窦手术中的出血量和能见度:一项随机临床试验。","authors":"Philip F Lavere, Nikunj A Rana, Michael P Kinsky, J Sean Funston, Sharif S Mohamed, Mohamad R Chaaban","doi":"10.1177/1179550619847992","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Improved intraoperative visibility during functional endoscopic sinus surgery (FESS) decreases the risk of serious orbital or skull base injuries. Esmolol and labetalol have been used to reduce bleeding and achieve better visibility, but it remains unclear which drug is more effective. This study aims to measure visibility scores and mucosal bleeding rates for esmolol and labetalol in FESS.</p><p><strong>Methods: </strong>This is a 1-year randomized double-blind trial of adults undergoing FESS at a tertiary academic center. The inclusion criteria were as follows: age 18 or older; history of chronic rhinosinusitis (CRS) with or without nasal polyps; undergoing FESS for CRS; and American Society of Anesthesiologists (ASA) physical status 1 (healthy) or 2 (patient with mild systemic disease). The exclusion criteria were as follows: pregnancy; asthma, chronic obstructive pulmonary disease (COPD), bradycardia, heart failure, end-stage renal disease, cerebrovascular accident, diabetes mellitus; preoperative use of nonsteroidal anti-inflammatory drugs (NSAIDs), aspirin, or beta-blockers; and body mass index (BMI) greater than 40 kg/m<sup>2</sup>. Patients received either dose-infused esmolol or intravenous push labetalol. The primary outcome was intraoperative visibility determined by surgeon using validated scoring systems (Boezaart, Wormald). The secondary outcome was hemodynamic control (rate of blood loss, average mean arterial pressure [MAP], average heart rate [HR]). Hypothesis of no difference between drugs formed before data collection.</p><p><strong>Results: </strong>Of the 32 adults given drug (mean age = 50), 28 patients (13 esmolol and 15 labetalol) with complete data were included in the final analysis. There were no statistically significant differences between esmolol and labetalol in rate of blood loss (0.59 [0.28] vs 0.66 [0.37] mL/min, <i>P</i> = 0.62), average MAP (79.7 [7.5] vs 79.4 [7.7] mm Hg, <i>P</i> = .93), HR (72 [8.7] vs 68 [11.7] bpm, <i>P</i> = .26), or mean visibility scores for the Boezaart (3.1 [0.69] vs 3.1 [0.89], <i>P</i> = .85) and Wormald (6.1 [1.7] vs 5.9 [1.9], <i>P</i> = .72) grading scales.</p><p><strong>Conclusions: </strong>There were no significant differences between esmolol and labetalol in rate of blood loss, MAP control, HR, or surgical visibility in FESS. Either drug may be used, and other considerations (availability, cost) can dictate choice.</p>","PeriodicalId":89906,"journal":{"name":"Clinical medicine insights. Ear, nose and throat","volume":"12 ","pages":"1179550619847992"},"PeriodicalIF":0.0000,"publicationDate":"2019-05-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1179550619847992","citationCount":"4","resultStr":"{\"title\":\"Blood Loss and Visibility with Esmolol vs Labetalol in Endoscopic Sinus Surgery: A Randomized Clinical Trial.\",\"authors\":\"Philip F Lavere, Nikunj A Rana, Michael P Kinsky, J Sean Funston, Sharif S Mohamed, Mohamad R Chaaban\",\"doi\":\"10.1177/1179550619847992\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Improved intraoperative visibility during functional endoscopic sinus surgery (FESS) decreases the risk of serious orbital or skull base injuries. Esmolol and labetalol have been used to reduce bleeding and achieve better visibility, but it remains unclear which drug is more effective. This study aims to measure visibility scores and mucosal bleeding rates for esmolol and labetalol in FESS.</p><p><strong>Methods: </strong>This is a 1-year randomized double-blind trial of adults undergoing FESS at a tertiary academic center. The inclusion criteria were as follows: age 18 or older; history of chronic rhinosinusitis (CRS) with or without nasal polyps; undergoing FESS for CRS; and American Society of Anesthesiologists (ASA) physical status 1 (healthy) or 2 (patient with mild systemic disease). The exclusion criteria were as follows: pregnancy; asthma, chronic obstructive pulmonary disease (COPD), bradycardia, heart failure, end-stage renal disease, cerebrovascular accident, diabetes mellitus; preoperative use of nonsteroidal anti-inflammatory drugs (NSAIDs), aspirin, or beta-blockers; and body mass index (BMI) greater than 40 kg/m<sup>2</sup>. Patients received either dose-infused esmolol or intravenous push labetalol. The primary outcome was intraoperative visibility determined by surgeon using validated scoring systems (Boezaart, Wormald). The secondary outcome was hemodynamic control (rate of blood loss, average mean arterial pressure [MAP], average heart rate [HR]). Hypothesis of no difference between drugs formed before data collection.</p><p><strong>Results: </strong>Of the 32 adults given drug (mean age = 50), 28 patients (13 esmolol and 15 labetalol) with complete data were included in the final analysis. There were no statistically significant differences between esmolol and labetalol in rate of blood loss (0.59 [0.28] vs 0.66 [0.37] mL/min, <i>P</i> = 0.62), average MAP (79.7 [7.5] vs 79.4 [7.7] mm Hg, <i>P</i> = .93), HR (72 [8.7] vs 68 [11.7] bpm, <i>P</i> = .26), or mean visibility scores for the Boezaart (3.1 [0.69] vs 3.1 [0.89], <i>P</i> = .85) and Wormald (6.1 [1.7] vs 5.9 [1.9], <i>P</i> = .72) grading scales.</p><p><strong>Conclusions: </strong>There were no significant differences between esmolol and labetalol in rate of blood loss, MAP control, HR, or surgical visibility in FESS. Either drug may be used, and other considerations (availability, cost) can dictate choice.</p>\",\"PeriodicalId\":89906,\"journal\":{\"name\":\"Clinical medicine insights. Ear, nose and throat\",\"volume\":\"12 \",\"pages\":\"1179550619847992\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2019-05-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1179550619847992\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical medicine insights. Ear, nose and throat\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1179550619847992\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical medicine insights. Ear, nose and throat","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179550619847992","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 4
摘要
目的:在功能性内窥镜鼻窦手术(FESS)中,提高术中能见度可降低严重眶或颅底损伤的风险。艾司洛尔和拉比他洛尔已被用于减少出血和提高能见度,但目前尚不清楚哪种药物更有效。本研究旨在测量艾司洛尔和拉贝他洛尔在FESS中的可视性评分和粘膜出血率。方法:这是一项为期1年的随机双盲试验,在一个三级学术中心接受FESS。纳入标准如下:18岁及以上;慢性鼻窦炎(CRS)病史,伴或不伴鼻息肉;为CRS接受FESS;美国麻醉医师协会(ASA)生理状态1(健康)或2(轻度全身性疾病患者)。排除标准如下:怀孕;哮喘、慢性阻塞性肺疾病(COPD)、心动过缓、心力衰竭、终末期肾病、脑血管意外、糖尿病;术前使用非甾体抗炎药(NSAIDs)、阿司匹林或受体阻滞剂;身体质量指数(BMI)大于40 kg/m2。患者接受剂量输注艾司洛尔或静脉推注拉贝他洛尔。主要结局是由外科医生使用有效的评分系统确定术中可见度(Boezaart, Wormald)。次要终点为血流动力学控制(出血率、平均动脉压(MAP)、平均心率(HR))。数据收集前形成药物间无差异的假设。结果:32例成人用药患者(平均年龄50岁)中,28例(艾司洛尔13例,拉贝他洛尔15例)资料完整纳入最终分析。艾司洛尔和拉贝他洛尔在失血率(0.59 [0.28]vs 0.66 [0.37] mL/min, P = 0.62)、平均MAP (79.7 [7.5] vs 79.4 [7.7] mm Hg, P = 0.93)、HR (72 [8.7] vs 68 [11.7] bpm, P = 0.26)、Boezaart评分(3.1 [0.69]vs 3.1 [0.89], P = 0.85)和Wormald评分(6.1 [1.7]vs 5.9 [1.9], P = 0.72)方面均无统计学差异。结论:艾司洛尔和拉贝他洛尔在FESS的出血率、MAP控制、HR或手术可见度方面无显著差异。任何一种药物都可以使用,其他考虑因素(可获得性、成本)可以决定选择。
Blood Loss and Visibility with Esmolol vs Labetalol in Endoscopic Sinus Surgery: A Randomized Clinical Trial.
Objectives: Improved intraoperative visibility during functional endoscopic sinus surgery (FESS) decreases the risk of serious orbital or skull base injuries. Esmolol and labetalol have been used to reduce bleeding and achieve better visibility, but it remains unclear which drug is more effective. This study aims to measure visibility scores and mucosal bleeding rates for esmolol and labetalol in FESS.
Methods: This is a 1-year randomized double-blind trial of adults undergoing FESS at a tertiary academic center. The inclusion criteria were as follows: age 18 or older; history of chronic rhinosinusitis (CRS) with or without nasal polyps; undergoing FESS for CRS; and American Society of Anesthesiologists (ASA) physical status 1 (healthy) or 2 (patient with mild systemic disease). The exclusion criteria were as follows: pregnancy; asthma, chronic obstructive pulmonary disease (COPD), bradycardia, heart failure, end-stage renal disease, cerebrovascular accident, diabetes mellitus; preoperative use of nonsteroidal anti-inflammatory drugs (NSAIDs), aspirin, or beta-blockers; and body mass index (BMI) greater than 40 kg/m2. Patients received either dose-infused esmolol or intravenous push labetalol. The primary outcome was intraoperative visibility determined by surgeon using validated scoring systems (Boezaart, Wormald). The secondary outcome was hemodynamic control (rate of blood loss, average mean arterial pressure [MAP], average heart rate [HR]). Hypothesis of no difference between drugs formed before data collection.
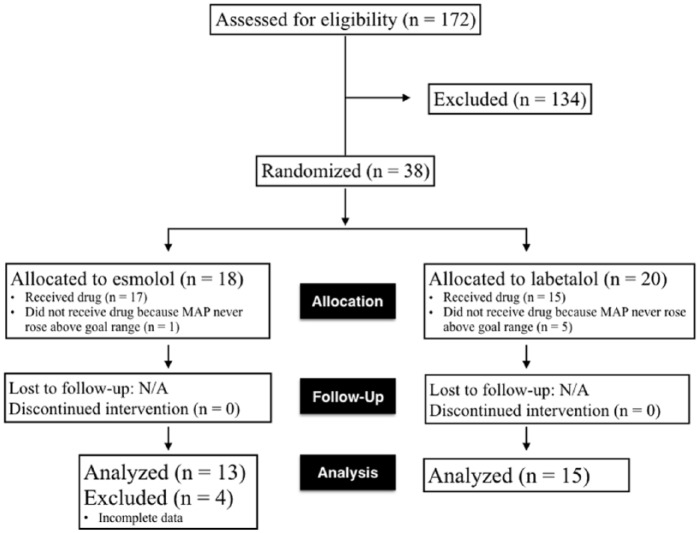
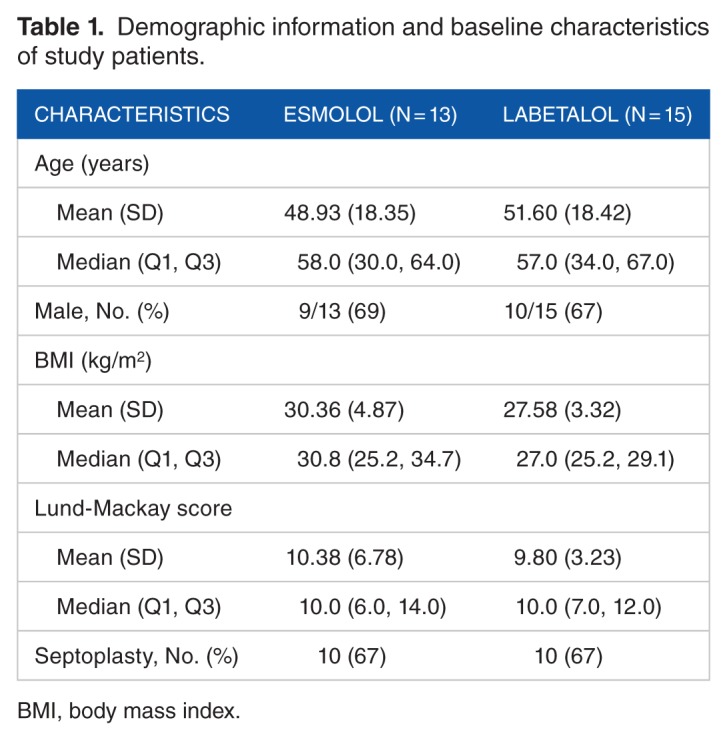
Results: Of the 32 adults given drug (mean age = 50), 28 patients (13 esmolol and 15 labetalol) with complete data were included in the final analysis. There were no statistically significant differences between esmolol and labetalol in rate of blood loss (0.59 [0.28] vs 0.66 [0.37] mL/min, P = 0.62), average MAP (79.7 [7.5] vs 79.4 [7.7] mm Hg, P = .93), HR (72 [8.7] vs 68 [11.7] bpm, P = .26), or mean visibility scores for the Boezaart (3.1 [0.69] vs 3.1 [0.89], P = .85) and Wormald (6.1 [1.7] vs 5.9 [1.9], P = .72) grading scales.
Conclusions: There were no significant differences between esmolol and labetalol in rate of blood loss, MAP control, HR, or surgical visibility in FESS. Either drug may be used, and other considerations (availability, cost) can dictate choice.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
