Ethan D Hinds, Manuel J Marin, Joggy George, Reynolds Delgado
{"title":"线圈栓塞治疗冠状动脉摄像瘘管。","authors":"Ethan D Hinds, Manuel J Marin, Joggy George, Reynolds Delgado","doi":"10.1177/2048004019856801","DOIUrl":null,"url":null,"abstract":"<p><p>A 56-year-old man who had twice previously undergone orthotopic heart transplantation was admitted with dyspnea and heart failure symptoms. A biopsy excluded rejection. Left heart catheterization revealed a coronary cameral fistula. After the patient was given mild diuretics, his condition improved. No significant fistula flow was detected, and he was discharged. Several months later, the patient was readmitted with worsening chest pain and dyspnea. Left ventricular end-diastolic pressure and flow through the fistula were increased. To correct the coronary cameral fistula, we performed a coil embolization without complications. Several months later at follow-up, the patient's symptoms had resolved, and his left ventricular end-diastolic pressure had normalized. We conclude that coronary fistulas may be caused by trauma to the heart during the de-airing process, which may be prevented in the future with the development of safer and more effective de-airing techniques.</p>","PeriodicalId":30457,"journal":{"name":"JRSM Cardiovascular Disease","volume":"8 ","pages":"2048004019856801"},"PeriodicalIF":1.5000,"publicationDate":"2019-06-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/2048004019856801","citationCount":"0","resultStr":"{\"title\":\"A coronary cameral fistula treated with coil embolization.\",\"authors\":\"Ethan D Hinds, Manuel J Marin, Joggy George, Reynolds Delgado\",\"doi\":\"10.1177/2048004019856801\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>A 56-year-old man who had twice previously undergone orthotopic heart transplantation was admitted with dyspnea and heart failure symptoms. A biopsy excluded rejection. Left heart catheterization revealed a coronary cameral fistula. After the patient was given mild diuretics, his condition improved. No significant fistula flow was detected, and he was discharged. Several months later, the patient was readmitted with worsening chest pain and dyspnea. Left ventricular end-diastolic pressure and flow through the fistula were increased. To correct the coronary cameral fistula, we performed a coil embolization without complications. Several months later at follow-up, the patient's symptoms had resolved, and his left ventricular end-diastolic pressure had normalized. We conclude that coronary fistulas may be caused by trauma to the heart during the de-airing process, which may be prevented in the future with the development of safer and more effective de-airing techniques.</p>\",\"PeriodicalId\":30457,\"journal\":{\"name\":\"JRSM Cardiovascular Disease\",\"volume\":\"8 \",\"pages\":\"2048004019856801\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2019-06-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/2048004019856801\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JRSM Cardiovascular Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/2048004019856801\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JRSM Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2048004019856801","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
A coronary cameral fistula treated with coil embolization.
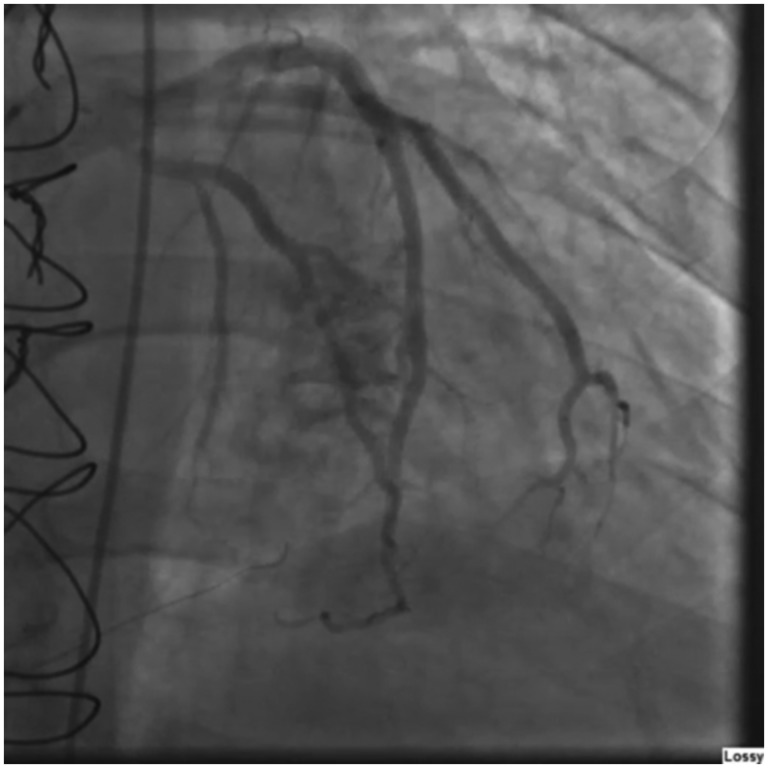
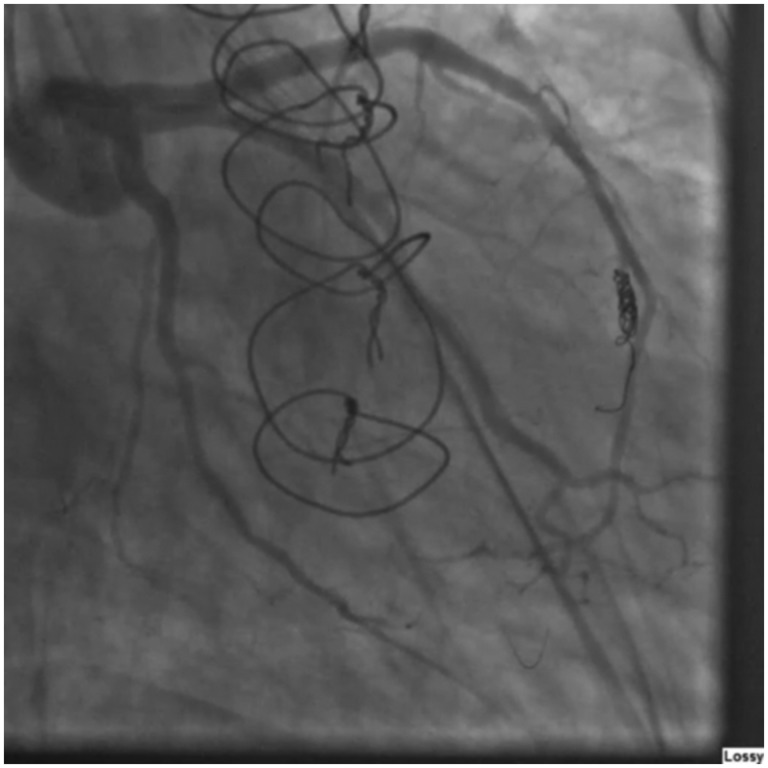
A 56-year-old man who had twice previously undergone orthotopic heart transplantation was admitted with dyspnea and heart failure symptoms. A biopsy excluded rejection. Left heart catheterization revealed a coronary cameral fistula. After the patient was given mild diuretics, his condition improved. No significant fistula flow was detected, and he was discharged. Several months later, the patient was readmitted with worsening chest pain and dyspnea. Left ventricular end-diastolic pressure and flow through the fistula were increased. To correct the coronary cameral fistula, we performed a coil embolization without complications. Several months later at follow-up, the patient's symptoms had resolved, and his left ventricular end-diastolic pressure had normalized. We conclude that coronary fistulas may be caused by trauma to the heart during the de-airing process, which may be prevented in the future with the development of safer and more effective de-airing techniques.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
