Florence Chamberlain, Sheima Farag, Constance Williams-Sharkey, Cecilia Collingwood, Lucia Chen, Sonia Mansukhani, Bodil Engelmann, Omar Al-Muderis, Dharmisha Chauhan, Khin Thway, Cyril Fisher, Robin L Jones, Spyridon Gennatas, Charlotte Benson
{"title":"一家三级癌症中心对胃肠道间质瘤(GIST)患者使用瑞戈非尼的毒性管理。","authors":"Florence Chamberlain, Sheima Farag, Constance Williams-Sharkey, Cecilia Collingwood, Lucia Chen, Sonia Mansukhani, Bodil Engelmann, Omar Al-Muderis, Dharmisha Chauhan, Khin Thway, Cyril Fisher, Robin L Jones, Spyridon Gennatas, Charlotte Benson","doi":"10.1186/s13569-019-0123-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Regorafenib is a multi-kinase inhibitor approved as third line treatment for metastatic GIST. Dose limiting toxicities are frequently seen and many patients require dose reductions. This study aimed to evaluate regorafenib toxicities and their management in a real-world GIST population.</p><p><strong>Methods: </strong>Retrospective review of a prospectively maintained database identified 50 patients with GIST treated with regorafenib at our centre between March 2013 and September 2018.</p><p><strong>Results: </strong>Median progression free survival (PFS) was 7.7 months [interquartile range (IQR) 2.8-14.4 months]. Median overall survival (OS) from start of regorafenib to death or last follow up was 15.7 months (IQR 9.2-28.4 months). Baseline median Eastern Cooperative Oncology Group (ECOG) performance status on starting regorafenib was 1. The main reason for discontinuing regorafenib was progressive disease (PD) (31/50 [62%]) rather than toxicity (10/50 [20%]). Grade 3-4 adverse events (AEs) were seen in 23/50 (46%) patients; palmar-plantar erythrodysesthesia (PPE) was most frequently seen (9/50 (18%)). Two patients died whilst on treatment with regorafenib from multi-organ failure secondary to sepsis (4%). Dose reductions were required in 19/50 patients (38%) and 8/50 (16%) patients started regorafenib at a lower dose band than the recommended dose (160 mg) due to comorbidities or concern over a higher individual risk of toxicity.</p><p><strong>Conclusion: </strong>Although PD was the main reason for discontinuing treatment, toxicity management and dosing of regorafenib remains critical. Median duration of treatment was longer compared to previous studies suggesting a durable clinical benefit with regorafenib with rigorous toxicity management.</p>","PeriodicalId":10684,"journal":{"name":"Clinical Sarcoma Research","volume":"10 ","pages":"1"},"PeriodicalIF":0.0000,"publicationDate":"2020-01-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6942401/pdf/","citationCount":"0","resultStr":"{\"title\":\"Toxicity management of regorafenib in patients with gastro-intestinal stromal tumour (GIST) in a tertiary cancer centre.\",\"authors\":\"Florence Chamberlain, Sheima Farag, Constance Williams-Sharkey, Cecilia Collingwood, Lucia Chen, Sonia Mansukhani, Bodil Engelmann, Omar Al-Muderis, Dharmisha Chauhan, Khin Thway, Cyril Fisher, Robin L Jones, Spyridon Gennatas, Charlotte Benson\",\"doi\":\"10.1186/s13569-019-0123-4\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Regorafenib is a multi-kinase inhibitor approved as third line treatment for metastatic GIST. Dose limiting toxicities are frequently seen and many patients require dose reductions. This study aimed to evaluate regorafenib toxicities and their management in a real-world GIST population.</p><p><strong>Methods: </strong>Retrospective review of a prospectively maintained database identified 50 patients with GIST treated with regorafenib at our centre between March 2013 and September 2018.</p><p><strong>Results: </strong>Median progression free survival (PFS) was 7.7 months [interquartile range (IQR) 2.8-14.4 months]. Median overall survival (OS) from start of regorafenib to death or last follow up was 15.7 months (IQR 9.2-28.4 months). Baseline median Eastern Cooperative Oncology Group (ECOG) performance status on starting regorafenib was 1. The main reason for discontinuing regorafenib was progressive disease (PD) (31/50 [62%]) rather than toxicity (10/50 [20%]). Grade 3-4 adverse events (AEs) were seen in 23/50 (46%) patients; palmar-plantar erythrodysesthesia (PPE) was most frequently seen (9/50 (18%)). Two patients died whilst on treatment with regorafenib from multi-organ failure secondary to sepsis (4%). Dose reductions were required in 19/50 patients (38%) and 8/50 (16%) patients started regorafenib at a lower dose band than the recommended dose (160 mg) due to comorbidities or concern over a higher individual risk of toxicity.</p><p><strong>Conclusion: </strong>Although PD was the main reason for discontinuing treatment, toxicity management and dosing of regorafenib remains critical. Median duration of treatment was longer compared to previous studies suggesting a durable clinical benefit with regorafenib with rigorous toxicity management.</p>\",\"PeriodicalId\":10684,\"journal\":{\"name\":\"Clinical Sarcoma Research\",\"volume\":\"10 \",\"pages\":\"1\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-01-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6942401/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Sarcoma Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13569-019-0123-4\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Sarcoma Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13569-019-0123-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Toxicity management of regorafenib in patients with gastro-intestinal stromal tumour (GIST) in a tertiary cancer centre.
Background: Regorafenib is a multi-kinase inhibitor approved as third line treatment for metastatic GIST. Dose limiting toxicities are frequently seen and many patients require dose reductions. This study aimed to evaluate regorafenib toxicities and their management in a real-world GIST population.
Methods: Retrospective review of a prospectively maintained database identified 50 patients with GIST treated with regorafenib at our centre between March 2013 and September 2018.
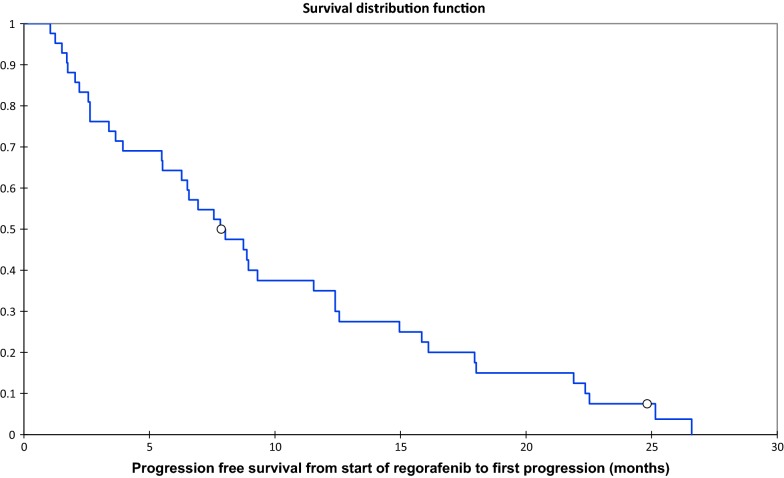
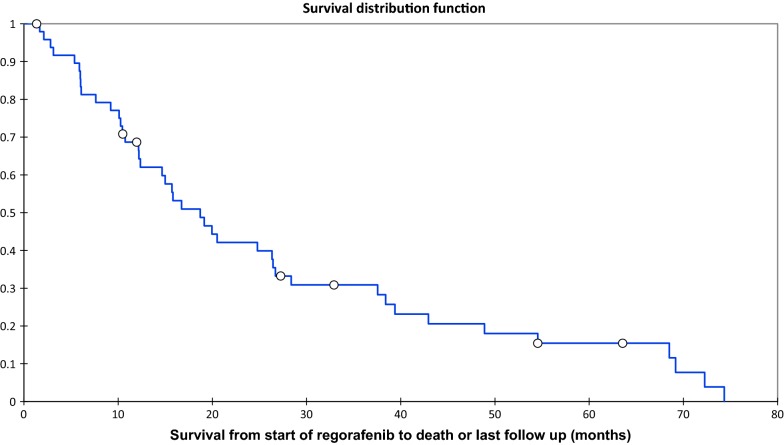
Results: Median progression free survival (PFS) was 7.7 months [interquartile range (IQR) 2.8-14.4 months]. Median overall survival (OS) from start of regorafenib to death or last follow up was 15.7 months (IQR 9.2-28.4 months). Baseline median Eastern Cooperative Oncology Group (ECOG) performance status on starting regorafenib was 1. The main reason for discontinuing regorafenib was progressive disease (PD) (31/50 [62%]) rather than toxicity (10/50 [20%]). Grade 3-4 adverse events (AEs) were seen in 23/50 (46%) patients; palmar-plantar erythrodysesthesia (PPE) was most frequently seen (9/50 (18%)). Two patients died whilst on treatment with regorafenib from multi-organ failure secondary to sepsis (4%). Dose reductions were required in 19/50 patients (38%) and 8/50 (16%) patients started regorafenib at a lower dose band than the recommended dose (160 mg) due to comorbidities or concern over a higher individual risk of toxicity.
Conclusion: Although PD was the main reason for discontinuing treatment, toxicity management and dosing of regorafenib remains critical. Median duration of treatment was longer compared to previous studies suggesting a durable clinical benefit with regorafenib with rigorous toxicity management.
期刊介绍:
Clinical Sarcoma Research considers for publication articles related to research on sarcomas, including both soft tissue and bone. The journal publishes original articles and review articles on the diagnosis and treatment of sarcomas along with new insights in sarcoma research, which may be of immediate or future interest for diagnosis and treatment. The journal also considers negative results, especially those from studies on new agents, as it is vital for the medical community to learn whether new agents have been proven effective or ineffective within subtypes of sarcomas. The journal also aims to offer a forum for active discussion on topics of major interest for the sarcoma community, which may be related to both research results and methodological topics.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
