Marrieth G Rubio, Kofi Amo-Mensah, James M Gray, Vu Q Nguyen, Sam Nakat, Douglas Grider, Kim Love, James H Boone, Dario Sorrentino
{"title":"粪乳铁蛋白准确反映炎症性肠病的粘膜炎症。","authors":"Marrieth G Rubio, Kofi Amo-Mensah, James M Gray, Vu Q Nguyen, Sam Nakat, Douglas Grider, Kim Love, James H Boone, Dario Sorrentino","doi":"10.4291/wjgp.v10.i5.54","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Studies have demonstrated a potential role for fecal biomarkers such as fecal calprotectin (FC) and fecal lactoferrin (FL) in monitoring inflammatory bowel diseases (IBD) - Crohn's disease (CD) and ulcerative colitis (UC). However, their correlation to endoscopic scores, disease severity and affected intestinal surface has not been extensively investigated.</p><p><strong>Aim: </strong>To correlate FL, and for comparison white blood cell (WBC) and C-reactive protein (CRP), with endoscopic scores, disease extent and location in CD and UC.</p><p><strong>Methods: </strong>Retrospective analysis in 188 patients who had FL, CRP and WBC determined within 30 d of endoscopy. Disease location, disease extent (number of intestinal segments involved), disease severity (determined by endoscopic scores), timing of FL testing in relation to colonoscopy, as well as the use of effective fast acting medications (steroids and biologics) between colonoscopy and FL measurement, were recorded.</p><p><strong>Results: </strong>In 131 CD and 57 UC patients, both CRP and FL - but not WBC - distinguished disease severity (inactive, mild, moderate, severe). In patients receiving fast-acting (steroids or biologics) treatment in between FL and colonoscopy, FL showed a higher correlation to endoscopic scores when tested before <i>vs</i> after the procedure (<i>r</i> = 0.596, <i>P</i> < 0.001, <i>vs r</i> = 0.285, <i>P</i> = 0.15 for the Simple Endoscopic Score for CD; and <i>r</i> = 0.402, <i>P</i> = 0.01 <i>vs r</i> = 0.054 <i>P</i> = 0.84 for Disease Activity Index). Finally, FL was significantly correlated with the diseased mucosal surface (colon-ileocolon > small bowel) and the number of inflamed colon segments.</p><p><strong>Conclusion: </strong>FL and CRP separated disease severity categories with FL showing lower discriminating <i>P</i>-values. FL showed a close correlation with the involved mucosal surface and with disease extent and was more closely correlated to endoscopy when determined before the procedure - this indicating that inflammatory activity changes associated with therapy might be rapidly reflected by FL levels. FL can accurately and timely characterize intestinal inflammation in IBD.</p>","PeriodicalId":23760,"journal":{"name":"World Journal of Gastrointestinal Pathophysiology","volume":"10 5","pages":"54-63"},"PeriodicalIF":0.0000,"publicationDate":"2019-12-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4f/be/WJGP-10-54.PMC6940564.pdf","citationCount":"14","resultStr":"{\"title\":\"Fecal lactoferrin accurately reflects mucosal inflammation in inflammatory bowel disease.\",\"authors\":\"Marrieth G Rubio, Kofi Amo-Mensah, James M Gray, Vu Q Nguyen, Sam Nakat, Douglas Grider, Kim Love, James H Boone, Dario Sorrentino\",\"doi\":\"10.4291/wjgp.v10.i5.54\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Studies have demonstrated a potential role for fecal biomarkers such as fecal calprotectin (FC) and fecal lactoferrin (FL) in monitoring inflammatory bowel diseases (IBD) - Crohn's disease (CD) and ulcerative colitis (UC). However, their correlation to endoscopic scores, disease severity and affected intestinal surface has not been extensively investigated.</p><p><strong>Aim: </strong>To correlate FL, and for comparison white blood cell (WBC) and C-reactive protein (CRP), with endoscopic scores, disease extent and location in CD and UC.</p><p><strong>Methods: </strong>Retrospective analysis in 188 patients who had FL, CRP and WBC determined within 30 d of endoscopy. Disease location, disease extent (number of intestinal segments involved), disease severity (determined by endoscopic scores), timing of FL testing in relation to colonoscopy, as well as the use of effective fast acting medications (steroids and biologics) between colonoscopy and FL measurement, were recorded.</p><p><strong>Results: </strong>In 131 CD and 57 UC patients, both CRP and FL - but not WBC - distinguished disease severity (inactive, mild, moderate, severe). In patients receiving fast-acting (steroids or biologics) treatment in between FL and colonoscopy, FL showed a higher correlation to endoscopic scores when tested before <i>vs</i> after the procedure (<i>r</i> = 0.596, <i>P</i> < 0.001, <i>vs r</i> = 0.285, <i>P</i> = 0.15 for the Simple Endoscopic Score for CD; and <i>r</i> = 0.402, <i>P</i> = 0.01 <i>vs r</i> = 0.054 <i>P</i> = 0.84 for Disease Activity Index). Finally, FL was significantly correlated with the diseased mucosal surface (colon-ileocolon > small bowel) and the number of inflamed colon segments.</p><p><strong>Conclusion: </strong>FL and CRP separated disease severity categories with FL showing lower discriminating <i>P</i>-values. FL showed a close correlation with the involved mucosal surface and with disease extent and was more closely correlated to endoscopy when determined before the procedure - this indicating that inflammatory activity changes associated with therapy might be rapidly reflected by FL levels. FL can accurately and timely characterize intestinal inflammation in IBD.</p>\",\"PeriodicalId\":23760,\"journal\":{\"name\":\"World Journal of Gastrointestinal Pathophysiology\",\"volume\":\"10 5\",\"pages\":\"54-63\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2019-12-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4f/be/WJGP-10-54.PMC6940564.pdf\",\"citationCount\":\"14\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Gastrointestinal Pathophysiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4291/wjgp.v10.i5.54\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Pathophysiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4291/wjgp.v10.i5.54","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 14
摘要
背景:研究已经证明粪便生物标志物如粪钙保护蛋白(FC)和粪乳铁蛋白(FL)在监测炎症性肠病(IBD) -克罗恩病(CD)和溃疡性结肠炎(UC)中的潜在作用。然而,它们与内镜评分、疾病严重程度和受影响肠表面的相关性尚未得到广泛研究。目的:将FL、白细胞(WBC)和c反应蛋白(CRP)与CD和UC的内镜评分、疾病程度和部位联系起来。方法:回顾性分析188例内镜检查后30 d内检测FL、CRP、WBC的患者。记录疾病位置、疾病程度(累及肠段数量)、疾病严重程度(由内窥镜评分决定)、与结肠镜检查相关的滤过膜检查时间,以及结肠镜检查和滤过膜测量之间有效的速效药物(类固醇和生物制剂)的使用情况。结果:在131例CD和57例UC患者中,CRP和FL(而非WBC)均可区分疾病严重程度(非活动性、轻度、中度、重度)。在FL和结肠镜检查之间接受速效(类固醇或生物制剂)治疗的患者,FL在术前和术后的内镜评分中显示出更高的相关性(r = 0.596, P < 0.001,对CD的简单内镜评分r = 0.285, P = 0.15);疾病活动指数r = 0.402, P = 0.01 vs r = 0.054 P = 0.84)。最后,FL与病变粘膜表面(结肠-回肠>小肠)和炎症结肠段数量显著相关。结论:FL与CRP区分疾病严重程度,FL具有较低的判别p值。FL与受损伤的粘膜表面和疾病程度密切相关,且术前确定与内镜检查更密切相关,这表明与治疗相关的炎症活动变化可能通过FL水平迅速反映。FL能准确、及时地表征IBD的肠道炎症。
Fecal lactoferrin accurately reflects mucosal inflammation in inflammatory bowel disease.
Background: Studies have demonstrated a potential role for fecal biomarkers such as fecal calprotectin (FC) and fecal lactoferrin (FL) in monitoring inflammatory bowel diseases (IBD) - Crohn's disease (CD) and ulcerative colitis (UC). However, their correlation to endoscopic scores, disease severity and affected intestinal surface has not been extensively investigated.
Aim: To correlate FL, and for comparison white blood cell (WBC) and C-reactive protein (CRP), with endoscopic scores, disease extent and location in CD and UC.
Methods: Retrospective analysis in 188 patients who had FL, CRP and WBC determined within 30 d of endoscopy. Disease location, disease extent (number of intestinal segments involved), disease severity (determined by endoscopic scores), timing of FL testing in relation to colonoscopy, as well as the use of effective fast acting medications (steroids and biologics) between colonoscopy and FL measurement, were recorded.
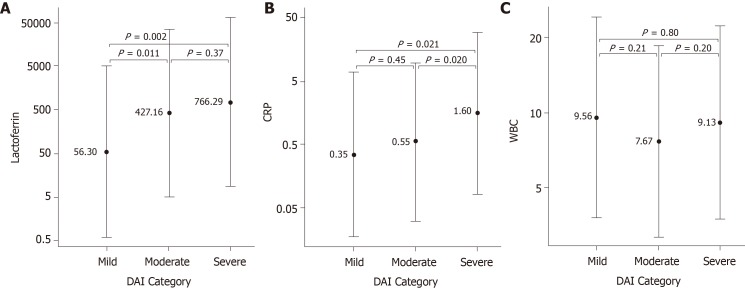
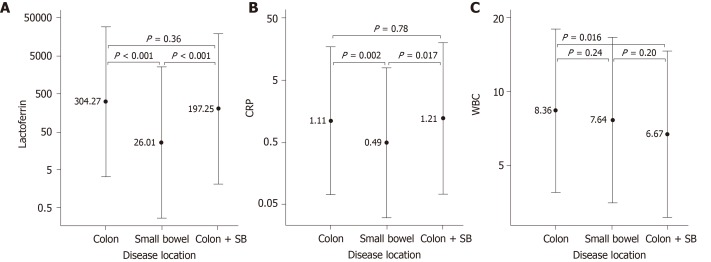
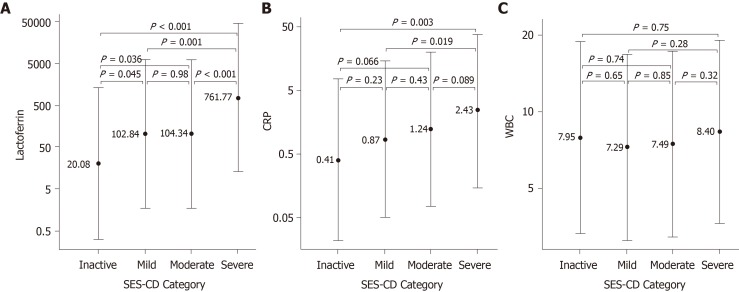
Results: In 131 CD and 57 UC patients, both CRP and FL - but not WBC - distinguished disease severity (inactive, mild, moderate, severe). In patients receiving fast-acting (steroids or biologics) treatment in between FL and colonoscopy, FL showed a higher correlation to endoscopic scores when tested before vs after the procedure (r = 0.596, P < 0.001, vs r = 0.285, P = 0.15 for the Simple Endoscopic Score for CD; and r = 0.402, P = 0.01 vs r = 0.054 P = 0.84 for Disease Activity Index). Finally, FL was significantly correlated with the diseased mucosal surface (colon-ileocolon > small bowel) and the number of inflamed colon segments.
Conclusion: FL and CRP separated disease severity categories with FL showing lower discriminating P-values. FL showed a close correlation with the involved mucosal surface and with disease extent and was more closely correlated to endoscopy when determined before the procedure - this indicating that inflammatory activity changes associated with therapy might be rapidly reflected by FL levels. FL can accurately and timely characterize intestinal inflammation in IBD.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
