John Barnard, Tyler Overholt, Ali Hajiran, Chad Crigger, Morris Jessop, Jennifer Knight, Chad Morley
{"title":"外伤性膀胱破裂:一级创伤中心十年回顾。","authors":"John Barnard, Tyler Overholt, Ali Hajiran, Chad Crigger, Morris Jessop, Jennifer Knight, Chad Morley","doi":"10.1155/2019/2614586","DOIUrl":null,"url":null,"abstract":"<p><p>Bladder rupture occurs in only 1.6% of blunt abdominopelvic trauma cases. Although rare, bladder rupture can result in significant morbidity if undiagnosed or inappropriately managed. AUA Urotrauma Guidelines suggest that urethral catheter drainage is a standard of care for both extraperitoneal and intraperitoneal bladder rupture regardless of the need for surgical repair. However, no specific guidance is given regarding the length of catheterization. The present study seeks to summarize contemporary management of bladder trauma at our tertiary care center, assess the impact of length of catheterization on bladder injuries and complications, and develop a protocol for management of bladder injuries from time of injury to catheter removal. A retrospective review was performed on 34,413 blunt trauma cases to identify traumatic bladder ruptures over the past 10 years (January 2008-January 2018) at our tertiary care facility. Patient data were collected including age, gender, BMI, mechanism of injury, and type of injury. The primary treatment modality (surgical repair vs. catheter drainage only), length of catheterization, and post-injury complications were also assessed. Review of our institutional trauma database identified 44 patients with bladder trauma. Mean age was 41 years, mean BMI was 24.8 kg/m<sup>2</sup>, 95% were Caucasian, and 55% were female. Motor vehicle collision (MVC) was the most common mechanism, representing 45% of total injuries. Other mechanisms included falls (20%) and all-terrain vehicle (ATV) accidents (13.6%). 31 patients had extraperitoneal injury, and 13 were intraperitoneal. Pelvic fractures were present in 93%, and 39% had additional solid organ injuries. Formal cystogram was performed in 59% on presentation, and mean time to cystogram was 4 hours. Gross hematuria was noted in 95% of cases. Operative management was performed for all intraperitoneal injuries and 35.5% of extraperitoneal cases. Bladder closure in operative cases was typically performed in 2 layers with absorbable suture in a running fashion. The intraperitoneal and extraperitoneal injuries managed operatively were compared, and length of catheterization (28 d vs. 22 d, <i>p</i>=0.46), time from injury to normal fluorocystogram (19.8 d vs. 20.7 d, <i>p</i>=0.80), and time from injury to repair (4.3 vs. 60.5 h, <i>p</i>=0.23) were not statistically different between cohorts. Patients whose catheter remained in place for greater than 14 days had prolonged time to initial cystogram (26.6 d vs. 11.5 d) compared with those whose foley catheter was removed within 14 days. The complication rate was 21% for catheters left more than 14 days while patients whose catheter remained less than 14 days experienced no complications. The present study provides a 10-year retrospective review characterizing the presentation, management, and follow-up of bladder trauma patients at our level 1 trauma center. Based on our findings, we have developed an institutional protocol which now includes recommendations regarding length of catheterization after traumatic bladder rupture. By providing specific guidelines for initial follow-up cystogram and foley removal, we hope to decrease patient morbidity from prolonged catheterization. Further study will seek to allow multidisciplinary trauma teams to standardize management, streamline care, and minimize complications for patients presenting with traumatic bladder injuries.</p>","PeriodicalId":7490,"journal":{"name":"Advances in Urology","volume":"2019 ","pages":"2614586"},"PeriodicalIF":2.3000,"publicationDate":"2019-12-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6930775/pdf/","citationCount":"0","resultStr":"{\"title\":\"Traumatic Bladder Ruptures: A Ten-Year Review at a Level 1 Trauma Center.\",\"authors\":\"John Barnard, Tyler Overholt, Ali Hajiran, Chad Crigger, Morris Jessop, Jennifer Knight, Chad Morley\",\"doi\":\"10.1155/2019/2614586\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Bladder rupture occurs in only 1.6% of blunt abdominopelvic trauma cases. Although rare, bladder rupture can result in significant morbidity if undiagnosed or inappropriately managed. AUA Urotrauma Guidelines suggest that urethral catheter drainage is a standard of care for both extraperitoneal and intraperitoneal bladder rupture regardless of the need for surgical repair. However, no specific guidance is given regarding the length of catheterization. The present study seeks to summarize contemporary management of bladder trauma at our tertiary care center, assess the impact of length of catheterization on bladder injuries and complications, and develop a protocol for management of bladder injuries from time of injury to catheter removal. A retrospective review was performed on 34,413 blunt trauma cases to identify traumatic bladder ruptures over the past 10 years (January 2008-January 2018) at our tertiary care facility. Patient data were collected including age, gender, BMI, mechanism of injury, and type of injury. The primary treatment modality (surgical repair vs. catheter drainage only), length of catheterization, and post-injury complications were also assessed. Review of our institutional trauma database identified 44 patients with bladder trauma. Mean age was 41 years, mean BMI was 24.8 kg/m<sup>2</sup>, 95% were Caucasian, and 55% were female. Motor vehicle collision (MVC) was the most common mechanism, representing 45% of total injuries. Other mechanisms included falls (20%) and all-terrain vehicle (ATV) accidents (13.6%). 31 patients had extraperitoneal injury, and 13 were intraperitoneal. Pelvic fractures were present in 93%, and 39% had additional solid organ injuries. Formal cystogram was performed in 59% on presentation, and mean time to cystogram was 4 hours. Gross hematuria was noted in 95% of cases. Operative management was performed for all intraperitoneal injuries and 35.5% of extraperitoneal cases. Bladder closure in operative cases was typically performed in 2 layers with absorbable suture in a running fashion. The intraperitoneal and extraperitoneal injuries managed operatively were compared, and length of catheterization (28 d vs. 22 d, <i>p</i>=0.46), time from injury to normal fluorocystogram (19.8 d vs. 20.7 d, <i>p</i>=0.80), and time from injury to repair (4.3 vs. 60.5 h, <i>p</i>=0.23) were not statistically different between cohorts. Patients whose catheter remained in place for greater than 14 days had prolonged time to initial cystogram (26.6 d vs. 11.5 d) compared with those whose foley catheter was removed within 14 days. The complication rate was 21% for catheters left more than 14 days while patients whose catheter remained less than 14 days experienced no complications. The present study provides a 10-year retrospective review characterizing the presentation, management, and follow-up of bladder trauma patients at our level 1 trauma center. Based on our findings, we have developed an institutional protocol which now includes recommendations regarding length of catheterization after traumatic bladder rupture. By providing specific guidelines for initial follow-up cystogram and foley removal, we hope to decrease patient morbidity from prolonged catheterization. Further study will seek to allow multidisciplinary trauma teams to standardize management, streamline care, and minimize complications for patients presenting with traumatic bladder injuries.</p>\",\"PeriodicalId\":7490,\"journal\":{\"name\":\"Advances in Urology\",\"volume\":\"2019 \",\"pages\":\"2614586\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2019-12-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6930775/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in Urology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2019/2614586\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2019/2614586","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
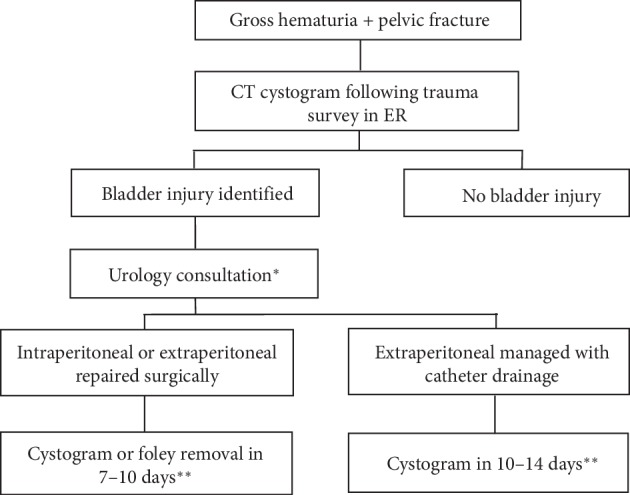
膀胱破裂仅发生在 1.6% 的腹盆腔钝性创伤病例中。膀胱破裂虽然罕见,但如果未得到诊断或处理不当,会导致严重的发病率。AUA 泌尿创伤指南建议,无论是否需要手术修复,尿道导管引流都是腹膜外和腹膜内膀胱破裂的标准治疗方法。但是,对于导尿时间的长短并没有给出具体的指导。本研究旨在总结我们三级医疗中心对膀胱创伤的当代管理方法,评估导尿时间对膀胱损伤和并发症的影响,并制定从损伤到拔除导尿管的膀胱损伤管理方案。我们对 34,413 例钝性外伤病例进行了回顾性审查,以确定过去 10 年(2008 年 1 月至 2018 年 1 月)在我们的三级医疗机构发生的外伤性膀胱破裂。收集的患者数据包括年龄、性别、体重指数、损伤机制和损伤类型。此外,还评估了主要治疗方式(手术修复与仅导管引流)、导管插入时间以及伤后并发症。通过查阅本机构的创伤数据库,共发现 44 名膀胱创伤患者。平均年龄为 41 岁,平均体重指数为 24.8 kg/m2,95% 为白种人,55% 为女性。机动车碰撞(MVC)是最常见的受伤机制,占总受伤人数的45%。其他原因包括摔伤(20%)和全地形车(ATV)事故(13.6%)。31例患者为腹膜外损伤,13例为腹膜内损伤。93%的患者有骨盆骨折,39%的患者有其他实体器官损伤。59%的患者在就诊时进行了正式的膀胱造影,膀胱造影的平均时间为4小时。95%的病例出现毛细血尿。所有腹膜内损伤和35.5%的腹膜外损伤病例均接受了手术治疗。手术病例的膀胱闭合一般分为两层,采用可吸收缝合线进行缝合。对腹膜内和腹膜外损伤的手术处理进行了比较,结果发现导尿时间(28 d vs. 22 d,p=0.46)、从损伤到膀胱荧光造影正常的时间(19.8 d vs. 20.7 d,p=0.80)以及从损伤到修复的时间(4.3 h vs. 60.5 h,p=0.23)在不同组别之间没有统计学差异。与 14 天内拔除导尿管的患者相比,导尿管留置时间超过 14 天的患者初次膀胱造影时间较长(26.6 天 vs. 11.5 天)。导尿管留置时间超过 14 天的患者并发症发生率为 21%,而导尿管留置时间少于 14 天的患者没有并发症发生。本研究对我们一级创伤中心的膀胱创伤患者的发病、管理和随访情况进行了为期 10 年的回顾性分析。根据我们的研究结果,我们制定了一项机构协议,其中包括关于外伤性膀胱破裂后导尿时间长短的建议。我们希望通过为初始随访膀胱造影和气管插管拔除提供具体指导,降低患者因长时间导尿而导致的发病率。进一步的研究将使多学科创伤团队能够对膀胱外伤患者进行标准化管理、简化护理并将并发症降至最低。
Traumatic Bladder Ruptures: A Ten-Year Review at a Level 1 Trauma Center.
Bladder rupture occurs in only 1.6% of blunt abdominopelvic trauma cases. Although rare, bladder rupture can result in significant morbidity if undiagnosed or inappropriately managed. AUA Urotrauma Guidelines suggest that urethral catheter drainage is a standard of care for both extraperitoneal and intraperitoneal bladder rupture regardless of the need for surgical repair. However, no specific guidance is given regarding the length of catheterization. The present study seeks to summarize contemporary management of bladder trauma at our tertiary care center, assess the impact of length of catheterization on bladder injuries and complications, and develop a protocol for management of bladder injuries from time of injury to catheter removal. A retrospective review was performed on 34,413 blunt trauma cases to identify traumatic bladder ruptures over the past 10 years (January 2008-January 2018) at our tertiary care facility. Patient data were collected including age, gender, BMI, mechanism of injury, and type of injury. The primary treatment modality (surgical repair vs. catheter drainage only), length of catheterization, and post-injury complications were also assessed. Review of our institutional trauma database identified 44 patients with bladder trauma. Mean age was 41 years, mean BMI was 24.8 kg/m2, 95% were Caucasian, and 55% were female. Motor vehicle collision (MVC) was the most common mechanism, representing 45% of total injuries. Other mechanisms included falls (20%) and all-terrain vehicle (ATV) accidents (13.6%). 31 patients had extraperitoneal injury, and 13 were intraperitoneal. Pelvic fractures were present in 93%, and 39% had additional solid organ injuries. Formal cystogram was performed in 59% on presentation, and mean time to cystogram was 4 hours. Gross hematuria was noted in 95% of cases. Operative management was performed for all intraperitoneal injuries and 35.5% of extraperitoneal cases. Bladder closure in operative cases was typically performed in 2 layers with absorbable suture in a running fashion. The intraperitoneal and extraperitoneal injuries managed operatively were compared, and length of catheterization (28 d vs. 22 d, p=0.46), time from injury to normal fluorocystogram (19.8 d vs. 20.7 d, p=0.80), and time from injury to repair (4.3 vs. 60.5 h, p=0.23) were not statistically different between cohorts. Patients whose catheter remained in place for greater than 14 days had prolonged time to initial cystogram (26.6 d vs. 11.5 d) compared with those whose foley catheter was removed within 14 days. The complication rate was 21% for catheters left more than 14 days while patients whose catheter remained less than 14 days experienced no complications. The present study provides a 10-year retrospective review characterizing the presentation, management, and follow-up of bladder trauma patients at our level 1 trauma center. Based on our findings, we have developed an institutional protocol which now includes recommendations regarding length of catheterization after traumatic bladder rupture. By providing specific guidelines for initial follow-up cystogram and foley removal, we hope to decrease patient morbidity from prolonged catheterization. Further study will seek to allow multidisciplinary trauma teams to standardize management, streamline care, and minimize complications for patients presenting with traumatic bladder injuries.
期刊介绍:
Advances in Urology is a peer-reviewed, open access journal that publishes state-of-the-art reviews and original research papers of wide interest in all fields of urology. The journal strives to provide publication of important manuscripts to the widest possible audience worldwide, without the constraints of expensive, hard-to-access, traditional bound journals. Advances in Urology is designed to improve publication access of both well-established urologic scientists and less well-established writers, by allowing interested scientists worldwide to participate fully.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
