E Dinoto, F Pecoraro, D Mirabella, F Ferlito, A Farina, N Lo Biundo, P Conti, G Bajardi
{"title":"药物洗脱球囊血管内治疗严重锁骨下动脉狭窄及椎动脉起源。","authors":"E Dinoto, F Pecoraro, D Mirabella, F Ferlito, A Farina, N Lo Biundo, P Conti, G Bajardi","doi":"","DOIUrl":null,"url":null,"abstract":"<p><p>The first line approach for subclavian steal syndrome is PTA-stenting of subclavian artery. When the ipsilateral vertebral artery origin is involved or in closed proximity of the atherosclerotic lesion in the subclavian artery PTA-stenting is at risk of ipsilateral vertebral artery coverage. Herein we report our experience with DEB to address lesions involving the subclavian artery and the origin of the ipsilateral vertebral artery. From January 2017 to February 2019, patients presenting subclavian artery lesion involving the origin of the ipsilateral vertebral artery and treated using primary DEB, were included. Three patients, with left subclavian steal syndrome, were identified. The perioperative mortality and morbidity were outcomes evaluated. Freedom from occlusion, secondary patency, amputation rate was registered. A total of 3 (2 female) patients were included in the study. No complication, symptoms recurrence, restenosis or occlusion were reported at duplex scan during 12-month follow-up. Indication for stenting was arterial dissection. In our limited experience, the use of DEB in association to embolic protection device in the treatment of atherosclerotic subclavian lesion involving the origin of the vertebral artery was safe and technically feasible.</p>","PeriodicalId":54170,"journal":{"name":"Translational Medicine at UniSa","volume":"21 ","pages":"35-37"},"PeriodicalIF":2.4000,"publicationDate":"2020-02-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7039271/pdf/","citationCount":"0","resultStr":"{\"title\":\"Endovascular Treatment with Drug-Eluting Balloon for Severe Subclavian Artery Stenosis Involving the Origin of the Vertebral Artery.\",\"authors\":\"E Dinoto, F Pecoraro, D Mirabella, F Ferlito, A Farina, N Lo Biundo, P Conti, G Bajardi\",\"doi\":\"\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>The first line approach for subclavian steal syndrome is PTA-stenting of subclavian artery. When the ipsilateral vertebral artery origin is involved or in closed proximity of the atherosclerotic lesion in the subclavian artery PTA-stenting is at risk of ipsilateral vertebral artery coverage. Herein we report our experience with DEB to address lesions involving the subclavian artery and the origin of the ipsilateral vertebral artery. From January 2017 to February 2019, patients presenting subclavian artery lesion involving the origin of the ipsilateral vertebral artery and treated using primary DEB, were included. Three patients, with left subclavian steal syndrome, were identified. The perioperative mortality and morbidity were outcomes evaluated. Freedom from occlusion, secondary patency, amputation rate was registered. A total of 3 (2 female) patients were included in the study. No complication, symptoms recurrence, restenosis or occlusion were reported at duplex scan during 12-month follow-up. Indication for stenting was arterial dissection. In our limited experience, the use of DEB in association to embolic protection device in the treatment of atherosclerotic subclavian lesion involving the origin of the vertebral artery was safe and technically feasible.</p>\",\"PeriodicalId\":54170,\"journal\":{\"name\":\"Translational Medicine at UniSa\",\"volume\":\"21 \",\"pages\":\"35-37\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2020-02-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7039271/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Translational Medicine at UniSa\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational Medicine at UniSa","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
Endovascular Treatment with Drug-Eluting Balloon for Severe Subclavian Artery Stenosis Involving the Origin of the Vertebral Artery.
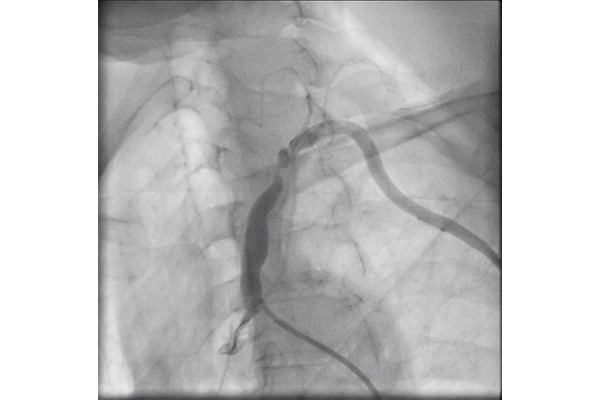
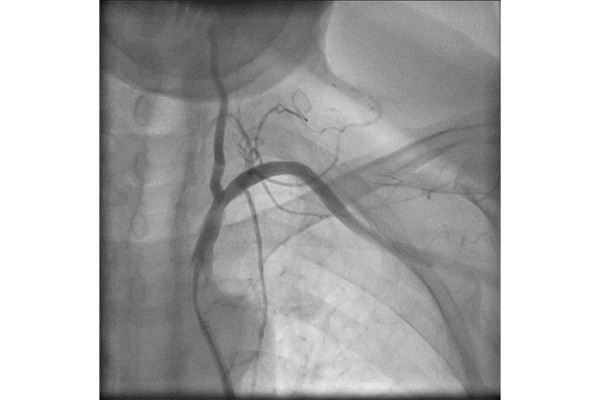
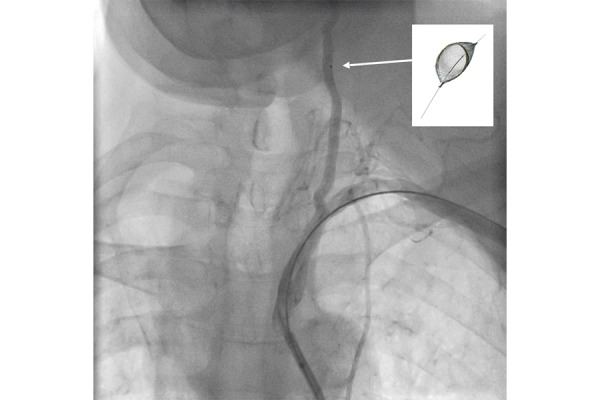
The first line approach for subclavian steal syndrome is PTA-stenting of subclavian artery. When the ipsilateral vertebral artery origin is involved or in closed proximity of the atherosclerotic lesion in the subclavian artery PTA-stenting is at risk of ipsilateral vertebral artery coverage. Herein we report our experience with DEB to address lesions involving the subclavian artery and the origin of the ipsilateral vertebral artery. From January 2017 to February 2019, patients presenting subclavian artery lesion involving the origin of the ipsilateral vertebral artery and treated using primary DEB, were included. Three patients, with left subclavian steal syndrome, were identified. The perioperative mortality and morbidity were outcomes evaluated. Freedom from occlusion, secondary patency, amputation rate was registered. A total of 3 (2 female) patients were included in the study. No complication, symptoms recurrence, restenosis or occlusion were reported at duplex scan during 12-month follow-up. Indication for stenting was arterial dissection. In our limited experience, the use of DEB in association to embolic protection device in the treatment of atherosclerotic subclavian lesion involving the origin of the vertebral artery was safe and technically feasible.
 分享
分享




 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
