Paul Edward Muckelt, E M Roos, M Stokes, S McDonough, D T Grønne, S Ewings, S T Skou
{"title":"合并症及其与个体健康状况的关系:23,892例初级保健膝关节和髋关节骨关节炎患者的横断面分析","authors":"Paul Edward Muckelt, E M Roos, M Stokes, S McDonough, D T Grønne, S Ewings, S T Skou","doi":"10.1177/2235042X20920456","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>Robust data on the impact of comorbidities on health in people with osteoarthritis (OA) are lacking, despite its potential importance for patient management. Objectives were to determine coexisting conditions in people with OA in primary care and whether more comorbidities were linked with individual health status.</p><p><strong>Methods: </strong>A retrospective analysis of 23,892 patients with knee and hip OA was conducted to determine comorbidities present (number/clusters) and how these linked with pain intensity (0-100), widespread pain (site numbers), medication usage (paracetamol, nonsteroidal anti-inflammatory drugs, opioids), quality of life EuroQol five dimension scale (EQ-5D), and physical function (walking speed) using independent <i>t</i>-tests or <i>χ</i> <sup>2</sup> test.</p><p><strong>Results: </strong>Sixty-two percent of people with OA treated in primary care had at least one comorbidity; hypertension (37%), heart disease (8%), and diabetes (7%) being most common. Outcome measures worsened with more comorbidities (0-4+ comorbidities); pain intensity [mean (SD)] 46(22)-57(21); number of painful sites 3.7(3.0)-6.3(5.4); quality of life 0.73(0.10)-0.63(0.15); walking speed 1.57 m/s (0.33)-1.24 m/s (0.31), while the proportion of people using pain medication increased from 0 to 2 comorbidities (58-69%; <i>p</i> < 0.001), with an increase in opioid use from 4.6% to 19.5% with more comorbidities (0-4+ comorbidities).</p><p><strong>Conclusion: </strong>Most people with knee or hip OA in primary care have at least one other long-term condition. A greater number of comorbidities is linked with worsening health, highlighting the importance of screening for comorbidities when treating patients with OA. It is important for clinicians to consider how OA treatments will interact and affect other common comorbidities.</p>","PeriodicalId":92071,"journal":{"name":"Journal of comorbidity","volume":"10 ","pages":"2235042X20920456"},"PeriodicalIF":0.0000,"publicationDate":"2020-05-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/55/b6/10.1177_2235042X20920456.PMC7238776.pdf","citationCount":"0","resultStr":"{\"title\":\"Comorbidities and their link with individual health status: A cross-sectional analysis of 23,892 people with knee and hip osteoarthritis from primary care.\",\"authors\":\"Paul Edward Muckelt, E M Roos, M Stokes, S McDonough, D T Grønne, S Ewings, S T Skou\",\"doi\":\"10.1177/2235042X20920456\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>Robust data on the impact of comorbidities on health in people with osteoarthritis (OA) are lacking, despite its potential importance for patient management. Objectives were to determine coexisting conditions in people with OA in primary care and whether more comorbidities were linked with individual health status.</p><p><strong>Methods: </strong>A retrospective analysis of 23,892 patients with knee and hip OA was conducted to determine comorbidities present (number/clusters) and how these linked with pain intensity (0-100), widespread pain (site numbers), medication usage (paracetamol, nonsteroidal anti-inflammatory drugs, opioids), quality of life EuroQol five dimension scale (EQ-5D), and physical function (walking speed) using independent <i>t</i>-tests or <i>χ</i> <sup>2</sup> test.</p><p><strong>Results: </strong>Sixty-two percent of people with OA treated in primary care had at least one comorbidity; hypertension (37%), heart disease (8%), and diabetes (7%) being most common. Outcome measures worsened with more comorbidities (0-4+ comorbidities); pain intensity [mean (SD)] 46(22)-57(21); number of painful sites 3.7(3.0)-6.3(5.4); quality of life 0.73(0.10)-0.63(0.15); walking speed 1.57 m/s (0.33)-1.24 m/s (0.31), while the proportion of people using pain medication increased from 0 to 2 comorbidities (58-69%; <i>p</i> < 0.001), with an increase in opioid use from 4.6% to 19.5% with more comorbidities (0-4+ comorbidities).</p><p><strong>Conclusion: </strong>Most people with knee or hip OA in primary care have at least one other long-term condition. A greater number of comorbidities is linked with worsening health, highlighting the importance of screening for comorbidities when treating patients with OA. It is important for clinicians to consider how OA treatments will interact and affect other common comorbidities.</p>\",\"PeriodicalId\":92071,\"journal\":{\"name\":\"Journal of comorbidity\",\"volume\":\"10 \",\"pages\":\"2235042X20920456\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-05-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/55/b6/10.1177_2235042X20920456.PMC7238776.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of comorbidity\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/2235042X20920456\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of comorbidity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2235042X20920456","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:尽管合并症对患者管理具有潜在的重要性,但关于骨关节炎(OA)患者的合并症对健康影响的可靠数据尚缺乏。目的是确定初级保健中OA患者的共存状况,以及是否更多的合并症与个人健康状况有关。方法:采用独立t检验或χ 2检验,对23,892例膝关节和髋部OA患者进行回顾性分析,确定存在的合并症(数量/聚类)以及这些合并症与疼痛强度(0-100)、广泛疼痛(部位数量)、药物使用(扑热息痛、非甾体抗炎药、阿片类药物)、生活质量EuroQol五维量表(EQ-5D)和身体功能(步行速度)的关系。结果:62%接受初级保健治疗的OA患者至少有一种合并症;高血压(37%)、心脏病(8%)和糖尿病(7%)是最常见的。结果指标恶化,合并症更多(0-4+合并症);疼痛强度[平均(SD)] 46(22)-57(21);疼痛部位数3.7(3.0)-6.3(5.4);生活质量0.73(0.10)-0.63(0.15);步行速度1.57 m/s (0.33)-1.24 m/s(0.31),同时使用止痛药的人群合并症比例从0增加到2 (58-69%);P < 0.001),阿片类药物的使用从4.6%增加到19.5%,并伴有更多的合并症(0-4+合并症)。结论:大多数初级保健的膝关节或髋关节OA患者至少有一种其他长期疾病。更多的合并症与健康恶化有关,这突出了在治疗OA患者时筛查合并症的重要性。对于临床医生来说,重要的是要考虑OA治疗如何相互作用并影响其他常见的合并症。
Comorbidities and their link with individual health status: A cross-sectional analysis of 23,892 people with knee and hip osteoarthritis from primary care.
Objectives: Robust data on the impact of comorbidities on health in people with osteoarthritis (OA) are lacking, despite its potential importance for patient management. Objectives were to determine coexisting conditions in people with OA in primary care and whether more comorbidities were linked with individual health status.
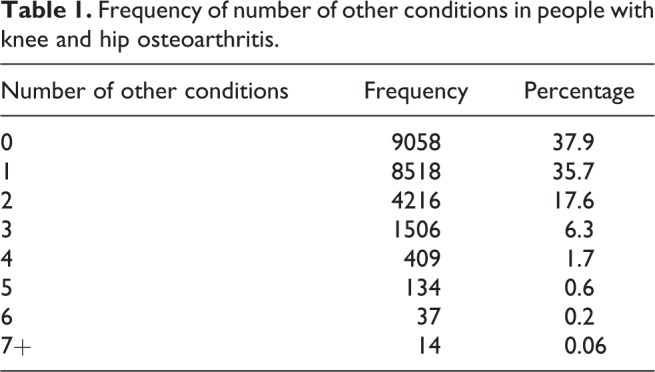
Methods: A retrospective analysis of 23,892 patients with knee and hip OA was conducted to determine comorbidities present (number/clusters) and how these linked with pain intensity (0-100), widespread pain (site numbers), medication usage (paracetamol, nonsteroidal anti-inflammatory drugs, opioids), quality of life EuroQol five dimension scale (EQ-5D), and physical function (walking speed) using independent t-tests or χ2 test.
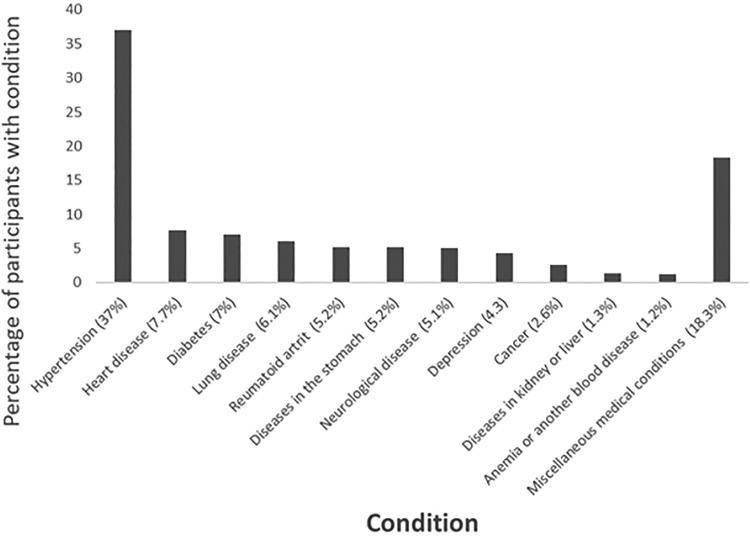
Results: Sixty-two percent of people with OA treated in primary care had at least one comorbidity; hypertension (37%), heart disease (8%), and diabetes (7%) being most common. Outcome measures worsened with more comorbidities (0-4+ comorbidities); pain intensity [mean (SD)] 46(22)-57(21); number of painful sites 3.7(3.0)-6.3(5.4); quality of life 0.73(0.10)-0.63(0.15); walking speed 1.57 m/s (0.33)-1.24 m/s (0.31), while the proportion of people using pain medication increased from 0 to 2 comorbidities (58-69%; p < 0.001), with an increase in opioid use from 4.6% to 19.5% with more comorbidities (0-4+ comorbidities).
Conclusion: Most people with knee or hip OA in primary care have at least one other long-term condition. A greater number of comorbidities is linked with worsening health, highlighting the importance of screening for comorbidities when treating patients with OA. It is important for clinicians to consider how OA treatments will interact and affect other common comorbidities.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
