John Ferguson, Michal Kazimir, Michael Gailey, Frank Moore, Earl Schott
{"title":"胸膜细胞学对复杂肺旁积液和胸脓肿诊断的预测价值。","authors":"John Ferguson, Michal Kazimir, Michael Gailey, Frank Moore, Earl Schott","doi":"10.1155/2020/7175451","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Complicated parapneumonic effusions (CPE) are distinguished from uncomplicated parapneumonic effusions (UPE) by the ability to resolve without drainage. Determinants include pleural pH, pleural glucose, and pleural LDH, along with microbiologic cultures. Inflammation mediated by neutrophil chemotactic cytokines leads to fibrinous loculation of an effusion, and the degree of this inflammation may lead to a CPE. One role of the pathologist is to evaluate for the presence of malignancy in a pleural effusion; however, the ability of the pathologist to distinguish a CPE from UPE has not been evaluated.</p><p><strong>Materials and methods: </strong>A single-center retrospective study was performed on pleural cytology specimens from 137 patients diagnosed with a parapneumonic effusion or empyema over a five-year interval. Pleural cytology was characterized as either uncomplicated or complicated by two pathologists based on cellular composition and the presence or absence of fibrinous exudate in the fluid. Cohen's kappa was calculated for interobserver agreement. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of cytologic diagnoses were calculated. Determinants of cytologic accuracy were assessed using Wilcoxon rank sum test, unpaired <i>t</i>-test, and logistic regression.</p><p><strong>Results: </strong>Kappa interobserver agreement between pathologists was 0.753. Pleural fluid cytology sensitivity, specificity, PPV, and NPV for CPE/empyema were 76.0%, 95% CI [65.0, 84.9]; 50%, 95% CI [29.1, 70.9]; 83.3%, 95% CI [76.7, 88.4]; and 38.7%, 95% CI [26.5, 52.5], respectively. The presence of pleural bacteria, elevated pleural LDH, and reduced pleural pH were nonsignificant determinants of cytologic accuracy. Logistic regression was significant for the presence of pleural bacteria (<i>p</i> = 0.03) in determining a successful cytologic diagnosis.</p><p><strong>Conclusion: </strong>Pleural cytology adds little value to traditional markers of distinguishing a UPE from CPE. Inflammation on pleural fluid cytology is suggestive of empyema or the presence of pleural fluid bacteria.</p>","PeriodicalId":46434,"journal":{"name":"Pulmonary Medicine","volume":"2020 ","pages":"7175451"},"PeriodicalIF":2.1000,"publicationDate":"2020-05-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/7175451","citationCount":"1","resultStr":"{\"title\":\"Predictive Value of Pleural Cytology in the Diagnosis of Complicated Parapneumonic Effusions and Empyema Thoracis.\",\"authors\":\"John Ferguson, Michal Kazimir, Michael Gailey, Frank Moore, Earl Schott\",\"doi\":\"10.1155/2020/7175451\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Complicated parapneumonic effusions (CPE) are distinguished from uncomplicated parapneumonic effusions (UPE) by the ability to resolve without drainage. Determinants include pleural pH, pleural glucose, and pleural LDH, along with microbiologic cultures. Inflammation mediated by neutrophil chemotactic cytokines leads to fibrinous loculation of an effusion, and the degree of this inflammation may lead to a CPE. One role of the pathologist is to evaluate for the presence of malignancy in a pleural effusion; however, the ability of the pathologist to distinguish a CPE from UPE has not been evaluated.</p><p><strong>Materials and methods: </strong>A single-center retrospective study was performed on pleural cytology specimens from 137 patients diagnosed with a parapneumonic effusion or empyema over a five-year interval. Pleural cytology was characterized as either uncomplicated or complicated by two pathologists based on cellular composition and the presence or absence of fibrinous exudate in the fluid. Cohen's kappa was calculated for interobserver agreement. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of cytologic diagnoses were calculated. Determinants of cytologic accuracy were assessed using Wilcoxon rank sum test, unpaired <i>t</i>-test, and logistic regression.</p><p><strong>Results: </strong>Kappa interobserver agreement between pathologists was 0.753. Pleural fluid cytology sensitivity, specificity, PPV, and NPV for CPE/empyema were 76.0%, 95% CI [65.0, 84.9]; 50%, 95% CI [29.1, 70.9]; 83.3%, 95% CI [76.7, 88.4]; and 38.7%, 95% CI [26.5, 52.5], respectively. The presence of pleural bacteria, elevated pleural LDH, and reduced pleural pH were nonsignificant determinants of cytologic accuracy. Logistic regression was significant for the presence of pleural bacteria (<i>p</i> = 0.03) in determining a successful cytologic diagnosis.</p><p><strong>Conclusion: </strong>Pleural cytology adds little value to traditional markers of distinguishing a UPE from CPE. Inflammation on pleural fluid cytology is suggestive of empyema or the presence of pleural fluid bacteria.</p>\",\"PeriodicalId\":46434,\"journal\":{\"name\":\"Pulmonary Medicine\",\"volume\":\"2020 \",\"pages\":\"7175451\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2020-05-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2020/7175451\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Pulmonary Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2020/7175451\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pulmonary Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/7175451","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 1
摘要
复杂性肺旁积液(CPE)与非复杂性肺旁积液(UPE)的区别在于其无需引流即可溶解。决定因素包括胸膜pH值,胸膜葡萄糖,胸膜乳酸脱氢酶,以及微生物培养。由中性粒细胞趋化细胞因子介导的炎症导致积液的纤维性定位,这种炎症的程度可能导致CPE。病理学家的作用之一是评估胸腔积液中是否存在恶性肿瘤;然而,病理学家区分CPE和UPE的能力尚未得到评估。材料和方法:对137例诊断为肺旁积液或脓胸的患者的胸膜细胞学标本进行了为期五年的单中心回顾性研究。根据细胞组成和液体中纤维性渗出物的存在与否,两名病理学家认为胸膜细胞学检查要么简单,要么复杂。科恩的kappa是根据观察者之间的一致计算的。计算细胞学诊断的敏感性、特异性、阳性预测值(PPV)和阴性预测值(NPV)。使用Wilcoxon秩和检验、非配对t检验和逻辑回归评估细胞学准确性的决定因素。结果:病理医师间Kappa观察者间一致性为0.753。胸膜液细胞学对CPE/脓胸的敏感性、特异性、PPV和NPV为76.0%,95% CI [65.0, 84.9];50%, 95% ci [29.1, 70.9];83.3%, 95% ci [76.7, 88.4];和38.7%,95% CI[26.5, 52.5]。胸膜细菌的存在、胸膜乳酸脱氢酶升高和胸膜pH值降低是细胞学准确性的非显著决定因素。逻辑回归在确定成功的细胞学诊断时,胸膜细菌的存在是显著的(p = 0.03)。结论:胸膜细胞学检查对传统的鉴别UPE和CPE的指标价值不大。胸膜液细胞学上的炎症提示有脓肿或胸膜液细菌的存在。
Predictive Value of Pleural Cytology in the Diagnosis of Complicated Parapneumonic Effusions and Empyema Thoracis.
Introduction: Complicated parapneumonic effusions (CPE) are distinguished from uncomplicated parapneumonic effusions (UPE) by the ability to resolve without drainage. Determinants include pleural pH, pleural glucose, and pleural LDH, along with microbiologic cultures. Inflammation mediated by neutrophil chemotactic cytokines leads to fibrinous loculation of an effusion, and the degree of this inflammation may lead to a CPE. One role of the pathologist is to evaluate for the presence of malignancy in a pleural effusion; however, the ability of the pathologist to distinguish a CPE from UPE has not been evaluated.
Materials and methods: A single-center retrospective study was performed on pleural cytology specimens from 137 patients diagnosed with a parapneumonic effusion or empyema over a five-year interval. Pleural cytology was characterized as either uncomplicated or complicated by two pathologists based on cellular composition and the presence or absence of fibrinous exudate in the fluid. Cohen's kappa was calculated for interobserver agreement. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of cytologic diagnoses were calculated. Determinants of cytologic accuracy were assessed using Wilcoxon rank sum test, unpaired t-test, and logistic regression.
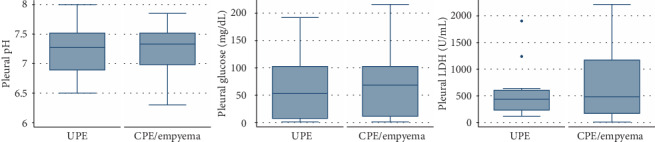
Results: Kappa interobserver agreement between pathologists was 0.753. Pleural fluid cytology sensitivity, specificity, PPV, and NPV for CPE/empyema were 76.0%, 95% CI [65.0, 84.9]; 50%, 95% CI [29.1, 70.9]; 83.3%, 95% CI [76.7, 88.4]; and 38.7%, 95% CI [26.5, 52.5], respectively. The presence of pleural bacteria, elevated pleural LDH, and reduced pleural pH were nonsignificant determinants of cytologic accuracy. Logistic regression was significant for the presence of pleural bacteria (p = 0.03) in determining a successful cytologic diagnosis.
Conclusion: Pleural cytology adds little value to traditional markers of distinguishing a UPE from CPE. Inflammation on pleural fluid cytology is suggestive of empyema or the presence of pleural fluid bacteria.






 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
