Megan L. Kavanaugh, Ayana Douglas-Hall, Sean M. Finn
{"title":"州一级的医疗保险覆盖率和避孕药具使用:2017年行为风险因素监测系统的调查结果","authors":"Megan L. Kavanaugh, Ayana Douglas-Hall, Sean M. Finn","doi":"10.1016/j.conx.2019.100014","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>To examine associations between health insurance coverage, income level and contraceptive use — overall and most/moderately effective method use — among women ages 18–44 at risk of pregnancy, within and across 41 United States jurisdictions in 2017.</p></div><div><h3>Study design</h3><p>Using data from the 2017 Behavioral Risk Factor Surveillance System, we calculated the proportions of women using any contraceptive method and using a most or moderately effective method for each state/territory and across all jurisdictions, categorized by health insurance coverage and income groups. For both contraceptive use outcomes, we ran simple and multivariable logistic regression models to test for significant differences in outcomes between insured and uninsured individuals.</p></div><div><h3>Results</h3><p>Across jurisdictions, compared to uninsured women, those who had health care coverage had higher levels of contraceptive use (65% versus 59%; p < .001) and most/moderately effective contraceptive use (43% compared to 35%; p < .001); low-income women with coverage also had higher levels of contraceptive use (64% versus 61%; p < .05) and most or moderately effective contraceptive use (42% versus 36%; p < .01) than their uninsured counterparts. Controlling for individual-level demographic characteristics, health insurance coverage was associated with increased odds of most or moderately effective contraceptive use across jurisdictions (adjusted odds ratio = 1.33, p < .01). In 11 states, insured women had significantly higher odds of at least one contraceptive use metric than their uninsured counterparts.</p></div><div><h3>Conclusions</h3><p>Variation in contraceptive use across the states likely reflects broader demographic, social and structural differences across state and local populations. States' political will and support around contraceptive access likely play a role in individuals' ability to obtain and use contraception.</p></div><div><h3>Implications</h3><p>Our key finding that insurance coverage is significantly associated with use of most/moderately effective contraceptive methods across the states but not any contraceptive use underscores the importance of health insurance in aiding access to methods that are more costly and often require a visit to a health care provider.</p></div>","PeriodicalId":10655,"journal":{"name":"Contraception: X","volume":"2 ","pages":"Article 100014"},"PeriodicalIF":0.0000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.conx.2019.100014","citationCount":"15","resultStr":"{\"title\":\"Health insurance coverage and contraceptive use at the state level: findings from the 2017 Behavioral Risk Factor Surveillance System\",\"authors\":\"Megan L. Kavanaugh, Ayana Douglas-Hall, Sean M. Finn\",\"doi\":\"10.1016/j.conx.2019.100014\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objective</h3><p>To examine associations between health insurance coverage, income level and contraceptive use — overall and most/moderately effective method use — among women ages 18–44 at risk of pregnancy, within and across 41 United States jurisdictions in 2017.</p></div><div><h3>Study design</h3><p>Using data from the 2017 Behavioral Risk Factor Surveillance System, we calculated the proportions of women using any contraceptive method and using a most or moderately effective method for each state/territory and across all jurisdictions, categorized by health insurance coverage and income groups. For both contraceptive use outcomes, we ran simple and multivariable logistic regression models to test for significant differences in outcomes between insured and uninsured individuals.</p></div><div><h3>Results</h3><p>Across jurisdictions, compared to uninsured women, those who had health care coverage had higher levels of contraceptive use (65% versus 59%; p < .001) and most/moderately effective contraceptive use (43% compared to 35%; p < .001); low-income women with coverage also had higher levels of contraceptive use (64% versus 61%; p < .05) and most or moderately effective contraceptive use (42% versus 36%; p < .01) than their uninsured counterparts. Controlling for individual-level demographic characteristics, health insurance coverage was associated with increased odds of most or moderately effective contraceptive use across jurisdictions (adjusted odds ratio = 1.33, p < .01). In 11 states, insured women had significantly higher odds of at least one contraceptive use metric than their uninsured counterparts.</p></div><div><h3>Conclusions</h3><p>Variation in contraceptive use across the states likely reflects broader demographic, social and structural differences across state and local populations. States' political will and support around contraceptive access likely play a role in individuals' ability to obtain and use contraception.</p></div><div><h3>Implications</h3><p>Our key finding that insurance coverage is significantly associated with use of most/moderately effective contraceptive methods across the states but not any contraceptive use underscores the importance of health insurance in aiding access to methods that are more costly and often require a visit to a health care provider.</p></div>\",\"PeriodicalId\":10655,\"journal\":{\"name\":\"Contraception: X\",\"volume\":\"2 \",\"pages\":\"Article 100014\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1016/j.conx.2019.100014\",\"citationCount\":\"15\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Contraception: X\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2590151619300139\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/11/15 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Contraception: X","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590151619300139","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/11/15 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Health insurance coverage and contraceptive use at the state level: findings from the 2017 Behavioral Risk Factor Surveillance System
Objective
To examine associations between health insurance coverage, income level and contraceptive use — overall and most/moderately effective method use — among women ages 18–44 at risk of pregnancy, within and across 41 United States jurisdictions in 2017.
Study design
Using data from the 2017 Behavioral Risk Factor Surveillance System, we calculated the proportions of women using any contraceptive method and using a most or moderately effective method for each state/territory and across all jurisdictions, categorized by health insurance coverage and income groups. For both contraceptive use outcomes, we ran simple and multivariable logistic regression models to test for significant differences in outcomes between insured and uninsured individuals.
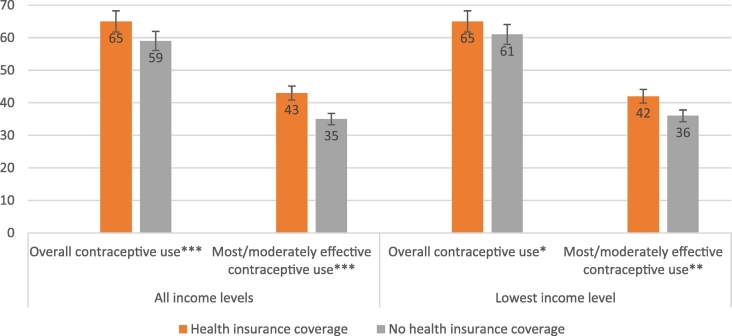
Results
Across jurisdictions, compared to uninsured women, those who had health care coverage had higher levels of contraceptive use (65% versus 59%; p < .001) and most/moderately effective contraceptive use (43% compared to 35%; p < .001); low-income women with coverage also had higher levels of contraceptive use (64% versus 61%; p < .05) and most or moderately effective contraceptive use (42% versus 36%; p < .01) than their uninsured counterparts. Controlling for individual-level demographic characteristics, health insurance coverage was associated with increased odds of most or moderately effective contraceptive use across jurisdictions (adjusted odds ratio = 1.33, p < .01). In 11 states, insured women had significantly higher odds of at least one contraceptive use metric than their uninsured counterparts.
Conclusions
Variation in contraceptive use across the states likely reflects broader demographic, social and structural differences across state and local populations. States' political will and support around contraceptive access likely play a role in individuals' ability to obtain and use contraception.
Implications
Our key finding that insurance coverage is significantly associated with use of most/moderately effective contraceptive methods across the states but not any contraceptive use underscores the importance of health insurance in aiding access to methods that are more costly and often require a visit to a health care provider.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
