D V Shchukin, V N Lesovoy, G G Khareba, A I Harahatyi, A V Maltsev, M M Polyakov, R V Stetsyshyn, M P Kopytsya, P V Mozzhakov, O O Makovozov
{"title":"非体外循环切除右心房肿瘤血栓:重点是肿瘤顶点的移位。","authors":"D V Shchukin, V N Lesovoy, G G Khareba, A I Harahatyi, A V Maltsev, M M Polyakov, R V Stetsyshyn, M P Kopytsya, P V Mozzhakov, O O Makovozov","doi":"10.1155/2020/6063018","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To assess the outcomes of cavoatrial tumor thrombus removal using the liver transplantation technique for thrombectomy, a retrospective study was conducted.</p><p><strong>Materials and methods: </strong>Five patients with atrial tumor thrombi who underwent piggy-back mobilization of the liver, surgical access to the right atrium from the abdominal cavity, and external manual repositioning of the thrombus apex below the diaphragm (milking maneuver) were included into the study. Extracorporeal circulation was used in none of the cases. The average length of the atrial component of the tumor was 20.0 ± 11.7 mm (10 to 35 mm), and the width was 14.8 ± 8.5 mm (10 to 30 mm). In this work, the features of patients and surgical interventions as well as perioperative complications and mortality were analyzed.</p><p><strong>Results: </strong>External manual repositioning of the tumor thrombus apex below the diaphragm was successfully performed in all patients. Tumor thrombi with the length of the atrial part up to 1.5 cm were removed through the extrapericardial approach. For evacuation of the thrombi with the large atrial part (3.0 cm or more), a transpericardial surgical approach was required. Specific complications associated with the access to the right atrium from the abdominal cavity (paresis of the right phrenic nerve, pneumothorax, and mediastinitis) were not detected in any case. The average clamping time of the supradiaphragmatic inferior vena cava (IVC) was 6.3 ± 4.6 min. The volume of intraoperative blood loss varied from 2500 to 5600 ml (an average of 3675 ± 1398.5 ml).</p><p><strong>Conclusion: </strong>Our work represents the initial experience in the liver transplantation technique for thrombectomy in distinct and well-selected patients with atrial tumor thrombi. The effectiveness of this approach needs further study. The video presentation of our research took place in March 2019 at the 34th Annual EAU Congress in Barcelona.</p>","PeriodicalId":7490,"journal":{"name":"Advances in Urology","volume":" ","pages":"6063018"},"PeriodicalIF":2.3000,"publicationDate":"2020-06-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/6063018","citationCount":"3","resultStr":"{\"title\":\"Removal of the Tumor Thrombus from the Right Atrium without Extracorporeal Circulation: Emphasis on the Displacement of the Tumor Apex.\",\"authors\":\"D V Shchukin, V N Lesovoy, G G Khareba, A I Harahatyi, A V Maltsev, M M Polyakov, R V Stetsyshyn, M P Kopytsya, P V Mozzhakov, O O Makovozov\",\"doi\":\"10.1155/2020/6063018\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To assess the outcomes of cavoatrial tumor thrombus removal using the liver transplantation technique for thrombectomy, a retrospective study was conducted.</p><p><strong>Materials and methods: </strong>Five patients with atrial tumor thrombi who underwent piggy-back mobilization of the liver, surgical access to the right atrium from the abdominal cavity, and external manual repositioning of the thrombus apex below the diaphragm (milking maneuver) were included into the study. Extracorporeal circulation was used in none of the cases. The average length of the atrial component of the tumor was 20.0 ± 11.7 mm (10 to 35 mm), and the width was 14.8 ± 8.5 mm (10 to 30 mm). In this work, the features of patients and surgical interventions as well as perioperative complications and mortality were analyzed.</p><p><strong>Results: </strong>External manual repositioning of the tumor thrombus apex below the diaphragm was successfully performed in all patients. Tumor thrombi with the length of the atrial part up to 1.5 cm were removed through the extrapericardial approach. For evacuation of the thrombi with the large atrial part (3.0 cm or more), a transpericardial surgical approach was required. Specific complications associated with the access to the right atrium from the abdominal cavity (paresis of the right phrenic nerve, pneumothorax, and mediastinitis) were not detected in any case. The average clamping time of the supradiaphragmatic inferior vena cava (IVC) was 6.3 ± 4.6 min. The volume of intraoperative blood loss varied from 2500 to 5600 ml (an average of 3675 ± 1398.5 ml).</p><p><strong>Conclusion: </strong>Our work represents the initial experience in the liver transplantation technique for thrombectomy in distinct and well-selected patients with atrial tumor thrombi. The effectiveness of this approach needs further study. The video presentation of our research took place in March 2019 at the 34th Annual EAU Congress in Barcelona.</p>\",\"PeriodicalId\":7490,\"journal\":{\"name\":\"Advances in Urology\",\"volume\":\" \",\"pages\":\"6063018\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2020-06-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2020/6063018\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in Urology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2020/6063018\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/6063018","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 3
摘要
目的:回顾性研究肝移植技术对腔房肿瘤血栓去除的效果。材料和方法:本研究纳入5例心房肿瘤血栓患者,均采用背扛式肝动员、腹腔手术进入右心房、体外手动将血栓顶端移至膈肌以下(挤乳手法)。所有病例均未采用体外循环。肿瘤心房部平均长20.0±11.7 mm (10 ~ 35 mm),宽14.8±8.5 mm (10 ~ 30 mm)。本文对患者特点、手术干预措施、围手术期并发症及死亡率进行分析。结果:所有患者均成功地完成了膈肌下肿瘤血栓顶端的手动复位。经心包外入路切除心房部长度达1.5 cm的肿瘤血栓。对于心房大部分(3.0 cm或以上)血栓的清除,需要经心包手术入路。从腹腔进入右心房的特殊并发症(右膈神经麻痹、气胸和纵隔炎)在任何病例中均未被发现。膈上下腔静脉(IVC)平均夹持时间为6.3±4.6 min。术中出血量2500 ~ 5600 ml(平均3675±1398.5 ml)。结论:我们的工作代表了肝移植技术在特殊和精心挑选的心房肿瘤血栓患者中取栓的初步经验。这种方法的有效性有待进一步研究。我们的研究于2019年3月在巴塞罗那举行的第34届欧亚联盟年度大会上进行了视频演示。
Removal of the Tumor Thrombus from the Right Atrium without Extracorporeal Circulation: Emphasis on the Displacement of the Tumor Apex.
Objectives: To assess the outcomes of cavoatrial tumor thrombus removal using the liver transplantation technique for thrombectomy, a retrospective study was conducted.
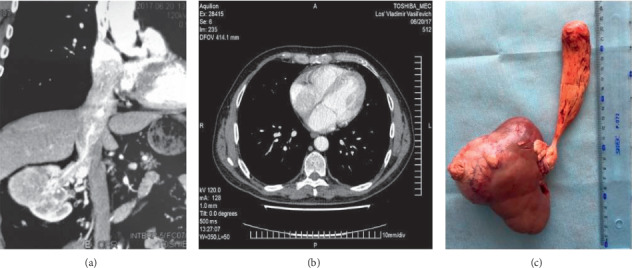
Materials and methods: Five patients with atrial tumor thrombi who underwent piggy-back mobilization of the liver, surgical access to the right atrium from the abdominal cavity, and external manual repositioning of the thrombus apex below the diaphragm (milking maneuver) were included into the study. Extracorporeal circulation was used in none of the cases. The average length of the atrial component of the tumor was 20.0 ± 11.7 mm (10 to 35 mm), and the width was 14.8 ± 8.5 mm (10 to 30 mm). In this work, the features of patients and surgical interventions as well as perioperative complications and mortality were analyzed.
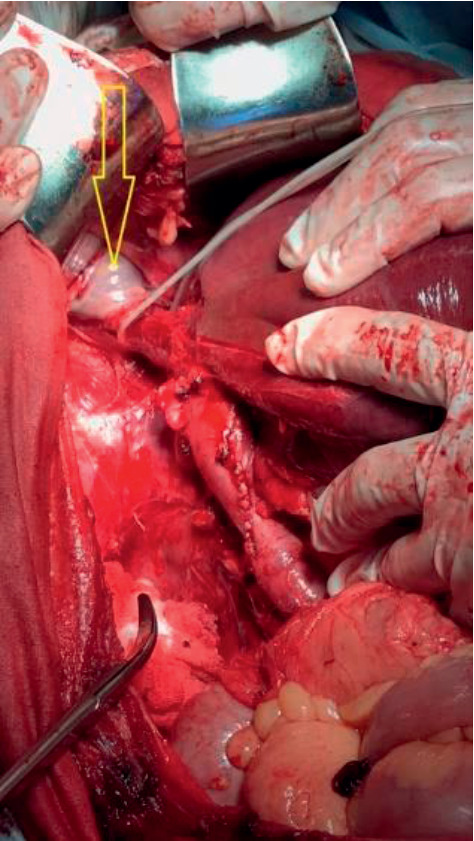
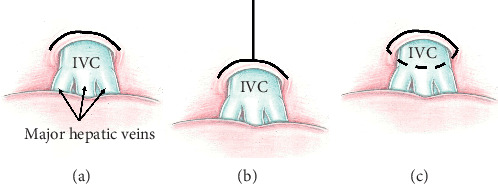
Results: External manual repositioning of the tumor thrombus apex below the diaphragm was successfully performed in all patients. Tumor thrombi with the length of the atrial part up to 1.5 cm were removed through the extrapericardial approach. For evacuation of the thrombi with the large atrial part (3.0 cm or more), a transpericardial surgical approach was required. Specific complications associated with the access to the right atrium from the abdominal cavity (paresis of the right phrenic nerve, pneumothorax, and mediastinitis) were not detected in any case. The average clamping time of the supradiaphragmatic inferior vena cava (IVC) was 6.3 ± 4.6 min. The volume of intraoperative blood loss varied from 2500 to 5600 ml (an average of 3675 ± 1398.5 ml).
Conclusion: Our work represents the initial experience in the liver transplantation technique for thrombectomy in distinct and well-selected patients with atrial tumor thrombi. The effectiveness of this approach needs further study. The video presentation of our research took place in March 2019 at the 34th Annual EAU Congress in Barcelona.
期刊介绍:
Advances in Urology is a peer-reviewed, open access journal that publishes state-of-the-art reviews and original research papers of wide interest in all fields of urology. The journal strives to provide publication of important manuscripts to the widest possible audience worldwide, without the constraints of expensive, hard-to-access, traditional bound journals. Advances in Urology is designed to improve publication access of both well-established urologic scientists and less well-established writers, by allowing interested scientists worldwide to participate fully.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
