Mayumi Ito, Takayuki Katsuno, Asako Kachi, Yasuhiko Ito
{"title":"以弥漫性肺泡出血和血栓性微血管病变为表现的高血压急症:1例报告及文献复习。","authors":"Mayumi Ito, Takayuki Katsuno, Asako Kachi, Yasuhiko Ito","doi":"10.5414/CNCS109939","DOIUrl":null,"url":null,"abstract":"<p><p>There are few studies reporting diffuse alveolar hemorrhage (DAH) caused by hypertensive emergency. We describe a 41-year-old man who visited the emergency room with hemoptysis and dyspnea. He had a 5-year history of hypertension, though he had not received any treatment. His blood pressure was 233/159 mmHg, his percutaneous oxygen saturation level was 88% on room air, and he had a serum creatinine level of 11.7 mg/dL. Laboratory data showed microangiopathic hemolytic anemia, thrombocytopenia, and severe kidney damage, suggesting thrombotic microangiopathy (TMA). Chest computed tomography and bronchoalveolar lavage revealed pulmonary alveolar hemorrhage. In addition to steroid treatment and plasma exchange, antihypertensive therapy was started immediately. On day 3, activity of a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13 (ADAMTS13) activity was not significantly reduced, and clinical markers for vasculitis and connective tissue disease were negative. Therefore, steroid administration and plasma exchange were discontinued. Although antihypertensive therapy centering on angiotensin II receptor blocker was effective for DAH and TMA, renal function did not recover, and maintenance hemodialysis was required. Renal pathological findings were consistent with malignant nephrosclerosis, and features suggestive of vasculitis were not found. The pathophysiology in this case was considered to be mainly hypertension and vascular endothelial injury with renin-angiotensin-aldosterone system (RAAS) activation. The use of RAAS inhibitor was effective in converging DAH and TMA, and it was expected to repair vascular endothelial damage associated with appropriate antihypertensive intervention. The authors present this rare condition with a review of previous reports.</p>","PeriodicalId":10398,"journal":{"name":"Clinical Nephrology. Case Studies","volume":"8 ","pages":"53-61"},"PeriodicalIF":0.0000,"publicationDate":"2020-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386058/pdf/","citationCount":"2","resultStr":"{\"title\":\"Hypertensive emergency presenting with diffuse alveolar hemorrhaging and thrombotic microangiopathy: A case report and review of the literature.\",\"authors\":\"Mayumi Ito, Takayuki Katsuno, Asako Kachi, Yasuhiko Ito\",\"doi\":\"10.5414/CNCS109939\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>There are few studies reporting diffuse alveolar hemorrhage (DAH) caused by hypertensive emergency. We describe a 41-year-old man who visited the emergency room with hemoptysis and dyspnea. He had a 5-year history of hypertension, though he had not received any treatment. His blood pressure was 233/159 mmHg, his percutaneous oxygen saturation level was 88% on room air, and he had a serum creatinine level of 11.7 mg/dL. Laboratory data showed microangiopathic hemolytic anemia, thrombocytopenia, and severe kidney damage, suggesting thrombotic microangiopathy (TMA). Chest computed tomography and bronchoalveolar lavage revealed pulmonary alveolar hemorrhage. In addition to steroid treatment and plasma exchange, antihypertensive therapy was started immediately. On day 3, activity of a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13 (ADAMTS13) activity was not significantly reduced, and clinical markers for vasculitis and connective tissue disease were negative. Therefore, steroid administration and plasma exchange were discontinued. Although antihypertensive therapy centering on angiotensin II receptor blocker was effective for DAH and TMA, renal function did not recover, and maintenance hemodialysis was required. Renal pathological findings were consistent with malignant nephrosclerosis, and features suggestive of vasculitis were not found. The pathophysiology in this case was considered to be mainly hypertension and vascular endothelial injury with renin-angiotensin-aldosterone system (RAAS) activation. The use of RAAS inhibitor was effective in converging DAH and TMA, and it was expected to repair vascular endothelial damage associated with appropriate antihypertensive intervention. The authors present this rare condition with a review of previous reports.</p>\",\"PeriodicalId\":10398,\"journal\":{\"name\":\"Clinical Nephrology. Case Studies\",\"volume\":\"8 \",\"pages\":\"53-61\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-07-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386058/pdf/\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Nephrology. Case Studies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5414/CNCS109939\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nephrology. Case Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS109939","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Hypertensive emergency presenting with diffuse alveolar hemorrhaging and thrombotic microangiopathy: A case report and review of the literature.
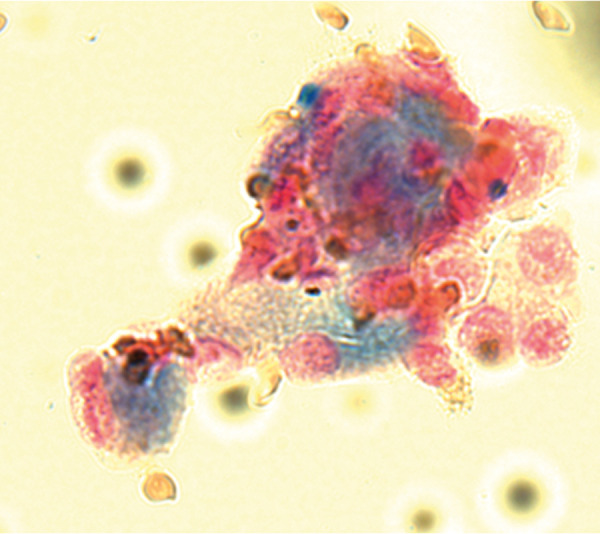
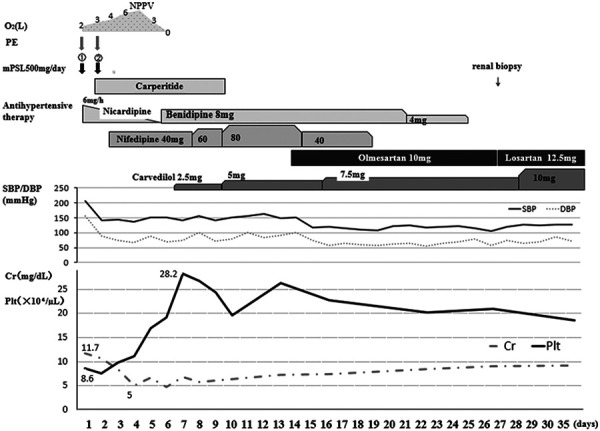
There are few studies reporting diffuse alveolar hemorrhage (DAH) caused by hypertensive emergency. We describe a 41-year-old man who visited the emergency room with hemoptysis and dyspnea. He had a 5-year history of hypertension, though he had not received any treatment. His blood pressure was 233/159 mmHg, his percutaneous oxygen saturation level was 88% on room air, and he had a serum creatinine level of 11.7 mg/dL. Laboratory data showed microangiopathic hemolytic anemia, thrombocytopenia, and severe kidney damage, suggesting thrombotic microangiopathy (TMA). Chest computed tomography and bronchoalveolar lavage revealed pulmonary alveolar hemorrhage. In addition to steroid treatment and plasma exchange, antihypertensive therapy was started immediately. On day 3, activity of a disintegrin and metalloproteinase with thrombospondin type 1 motif, member 13 (ADAMTS13) activity was not significantly reduced, and clinical markers for vasculitis and connective tissue disease were negative. Therefore, steroid administration and plasma exchange were discontinued. Although antihypertensive therapy centering on angiotensin II receptor blocker was effective for DAH and TMA, renal function did not recover, and maintenance hemodialysis was required. Renal pathological findings were consistent with malignant nephrosclerosis, and features suggestive of vasculitis were not found. The pathophysiology in this case was considered to be mainly hypertension and vascular endothelial injury with renin-angiotensin-aldosterone system (RAAS) activation. The use of RAAS inhibitor was effective in converging DAH and TMA, and it was expected to repair vascular endothelial damage associated with appropriate antihypertensive intervention. The authors present this rare condition with a review of previous reports.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
