Madeline B Libin, Joel G Weltman, Jennifer Prittie
{"title":"氯离子浓度与住院犬患者发病率和死亡率关系的初步调查。","authors":"Madeline B Libin, Joel G Weltman, Jennifer Prittie","doi":"10.2147/VMRR.S253759","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To evaluate whole blood chloride concentration and hospital-acquired AKI in hospitalized canine patients. Secondary outcome measures included the volume-adjusted chloride load, in-hospital mortality and length of ICU stay.</p><p><strong>Patients and methods: </strong>This is a prospective, observational study. Sixty dogs admitted to the ICU and receiving IV fluid therapy for >24 hours from February 2018 to July 2019. Corrected chloride and creatinine concentrations were obtained twice daily. Total volume of IV fluid and total chloride load were recorded. Volume-adjusted chloride load (VACL) was calculated by dividing the chloride administered by the volume of fluid administered. Hospital-acquired AKI was defined as an increase in creatinine of ≥26.5 μmol/L (0.3 mg/dL) or 150% from baseline to maximum. Survival to hospital discharge or non-survival and ICU length of stay were also recorded.</p><p><strong>Results: </strong>Fifteen out of 60 patients developed hospital-acquired AKI. Maximum corrected chloride was significantly different in AKI group (median 122.3 mmol/L) vs non-AKI group (median 118.1 mmol/L; p=0.0002). Six out of 60 patients developed hyperchloremia. Hyperchloremic patients were significantly more likely to develop in-hospital AKI (p=0.03). Patients hospitalized ≥2 days had a significantly higher [Cl<sup>-</sup>]<sub>max</sub> compared to those with shorter ICU stay (121.8 ± 5.9 mmol/L vs 117.5 ± 4.3 mmol/L; p=0.002). Eight out of 60 patients were non-survivors. Maximum corrected chloride and creatinine concentrations were not significantly different between survivors and non-survivors. VACL was not significantly different between AKI or mortality groups.</p><p><strong>Conclusion: </strong>Maximum corrected chloride concentration was significantly higher in dogs with hospital-acquired AKI, even amongst dogs without hyperchloremia. Additionally, maximum corrected chloride concentrations were significantly higher in dogs hospitalized in the ICU longer compared to those hospitalized for fewer than two days. There was no significant difference in VACL in any of the outcome groups. Results from this study suggest alterations in chloride may be observed alongside the development of acute kidney injuries. Future studies in critically ill dogs are warranted.</p>","PeriodicalId":75300,"journal":{"name":"Veterinary medicine (Auckland, N.Z.)","volume":"11 ","pages":"57-69"},"PeriodicalIF":2.5000,"publicationDate":"2020-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/VMRR.S253759","citationCount":"1","resultStr":"{\"title\":\"A Preliminary Investigation into the Association of Chloride Concentration on Morbidity and Mortality in Hospitalized Canine Patients.\",\"authors\":\"Madeline B Libin, Joel G Weltman, Jennifer Prittie\",\"doi\":\"10.2147/VMRR.S253759\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>To evaluate whole blood chloride concentration and hospital-acquired AKI in hospitalized canine patients. Secondary outcome measures included the volume-adjusted chloride load, in-hospital mortality and length of ICU stay.</p><p><strong>Patients and methods: </strong>This is a prospective, observational study. Sixty dogs admitted to the ICU and receiving IV fluid therapy for >24 hours from February 2018 to July 2019. Corrected chloride and creatinine concentrations were obtained twice daily. Total volume of IV fluid and total chloride load were recorded. Volume-adjusted chloride load (VACL) was calculated by dividing the chloride administered by the volume of fluid administered. Hospital-acquired AKI was defined as an increase in creatinine of ≥26.5 μmol/L (0.3 mg/dL) or 150% from baseline to maximum. Survival to hospital discharge or non-survival and ICU length of stay were also recorded.</p><p><strong>Results: </strong>Fifteen out of 60 patients developed hospital-acquired AKI. Maximum corrected chloride was significantly different in AKI group (median 122.3 mmol/L) vs non-AKI group (median 118.1 mmol/L; p=0.0002). Six out of 60 patients developed hyperchloremia. Hyperchloremic patients were significantly more likely to develop in-hospital AKI (p=0.03). Patients hospitalized ≥2 days had a significantly higher [Cl<sup>-</sup>]<sub>max</sub> compared to those with shorter ICU stay (121.8 ± 5.9 mmol/L vs 117.5 ± 4.3 mmol/L; p=0.002). Eight out of 60 patients were non-survivors. Maximum corrected chloride and creatinine concentrations were not significantly different between survivors and non-survivors. VACL was not significantly different between AKI or mortality groups.</p><p><strong>Conclusion: </strong>Maximum corrected chloride concentration was significantly higher in dogs with hospital-acquired AKI, even amongst dogs without hyperchloremia. Additionally, maximum corrected chloride concentrations were significantly higher in dogs hospitalized in the ICU longer compared to those hospitalized for fewer than two days. There was no significant difference in VACL in any of the outcome groups. Results from this study suggest alterations in chloride may be observed alongside the development of acute kidney injuries. Future studies in critically ill dogs are warranted.</p>\",\"PeriodicalId\":75300,\"journal\":{\"name\":\"Veterinary medicine (Auckland, N.Z.)\",\"volume\":\"11 \",\"pages\":\"57-69\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2020-07-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.2147/VMRR.S253759\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Veterinary medicine (Auckland, N.Z.)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/VMRR.S253759\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"VETERINARY SCIENCES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Veterinary medicine (Auckland, N.Z.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/VMRR.S253759","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"VETERINARY SCIENCES","Score":null,"Total":0}
A Preliminary Investigation into the Association of Chloride Concentration on Morbidity and Mortality in Hospitalized Canine Patients.
Purpose: To evaluate whole blood chloride concentration and hospital-acquired AKI in hospitalized canine patients. Secondary outcome measures included the volume-adjusted chloride load, in-hospital mortality and length of ICU stay.
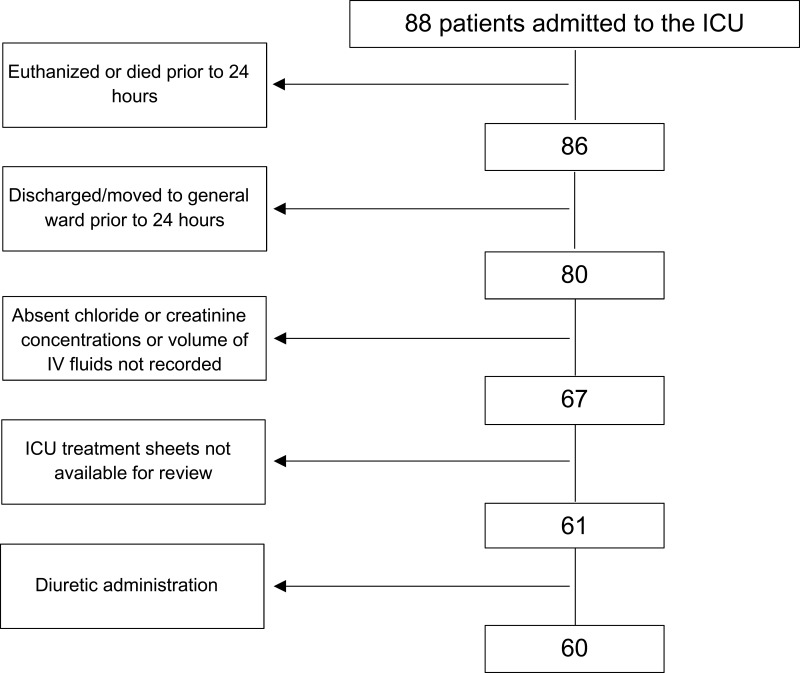
Patients and methods: This is a prospective, observational study. Sixty dogs admitted to the ICU and receiving IV fluid therapy for >24 hours from February 2018 to July 2019. Corrected chloride and creatinine concentrations were obtained twice daily. Total volume of IV fluid and total chloride load were recorded. Volume-adjusted chloride load (VACL) was calculated by dividing the chloride administered by the volume of fluid administered. Hospital-acquired AKI was defined as an increase in creatinine of ≥26.5 μmol/L (0.3 mg/dL) or 150% from baseline to maximum. Survival to hospital discharge or non-survival and ICU length of stay were also recorded.
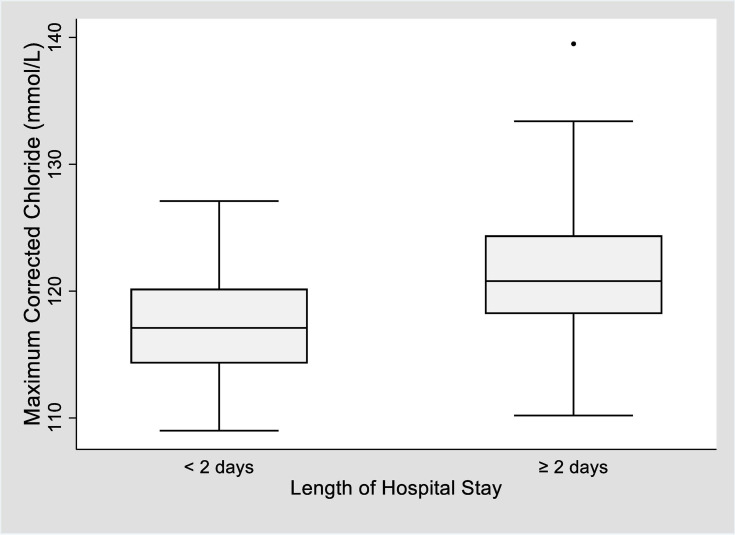
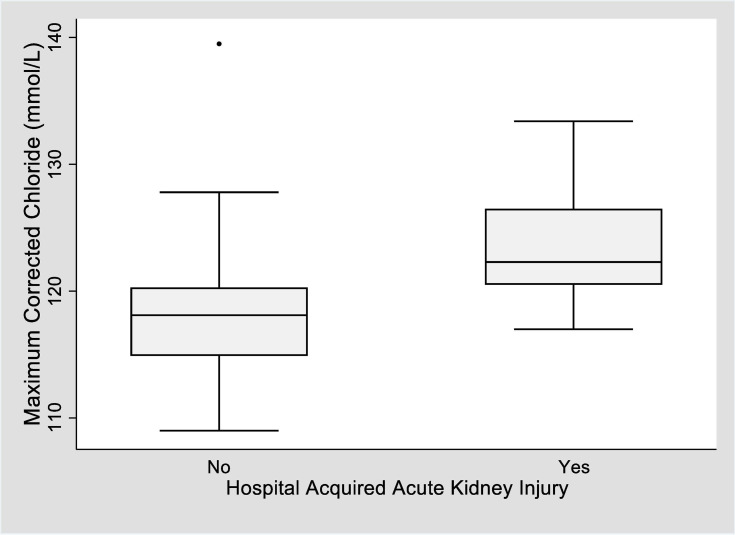
Results: Fifteen out of 60 patients developed hospital-acquired AKI. Maximum corrected chloride was significantly different in AKI group (median 122.3 mmol/L) vs non-AKI group (median 118.1 mmol/L; p=0.0002). Six out of 60 patients developed hyperchloremia. Hyperchloremic patients were significantly more likely to develop in-hospital AKI (p=0.03). Patients hospitalized ≥2 days had a significantly higher [Cl-]max compared to those with shorter ICU stay (121.8 ± 5.9 mmol/L vs 117.5 ± 4.3 mmol/L; p=0.002). Eight out of 60 patients were non-survivors. Maximum corrected chloride and creatinine concentrations were not significantly different between survivors and non-survivors. VACL was not significantly different between AKI or mortality groups.
Conclusion: Maximum corrected chloride concentration was significantly higher in dogs with hospital-acquired AKI, even amongst dogs without hyperchloremia. Additionally, maximum corrected chloride concentrations were significantly higher in dogs hospitalized in the ICU longer compared to those hospitalized for fewer than two days. There was no significant difference in VACL in any of the outcome groups. Results from this study suggest alterations in chloride may be observed alongside the development of acute kidney injuries. Future studies in critically ill dogs are warranted.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
