{"title":"重复经尿道切除术仍然是治疗非肌肉浸润性膀胱癌的重要工具:西澳大利亚经验。","authors":"Dwayne T S Chang, Alarick Picardo","doi":"10.14440/bladder.2020.814","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To determine the rate of residual disease and under-staging after primary transurethral resection (TUR) of bladder tumors (TURBT) in tertiary hospitals in Western Australia.</p><p><strong>Methods: </strong>A retrospective study was performed evaluating all patients with TaHG (stage Ta, high-grade), T1LG (stage T1, low-grade) or T1HG (stage T1, high-grade) bladder cancer on primary TURBT conducted between January 1, 2012 and December 31, 2017 at the four largest metropolitan public hospitals in Western Australia. Only patients who underwent repeat resection within 3 months from initial resection were included. Those with previous history of bladder cancer, incomplete follow-up data and visibly incomplete initial resection were excluded. Baseline patient demographics, macroscopic clearance at initial resection, and disease data at initial and repeat resections were recorded.</p><p><strong>Results: </strong>Sixty-seven patients with a median age of 71 years were included in this study. At initial resection, T1HG was the most common disease stage (64.2%) and detrusor muscle was present in 82.1% of initial resections. At repeat resection, 41.8% of cases had residual disease. The rate of upstaging to muscle-invasive bladder cancer was 3.0%. Patients treated by operators with five or less years of formal training did not have a significantly different rate of residual disease from patients treated by operators with more than five years of experience.</p><p><strong>Conclusions: </strong>Repeat TUR should remain an essential practice due to high rates of residual disease and a small risk of tumor under-staging. The presence of detrusor muscle and macroscopic clearance should not be used as surrogates for adequacy of resection or consideration of avoiding a repeat TUR, even for TaHG disease.</p>","PeriodicalId":72421,"journal":{"name":"Bladder (San Francisco, Calif.)","volume":"7 2","pages":"e42"},"PeriodicalIF":0.0000,"publicationDate":"2020-04-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/16/d1/bladder-7-2-e42.PMC7401982.pdf","citationCount":"4","resultStr":"{\"title\":\"Repeat transurethral resection is still an essential tool in treating non-muscle invasive bladder cancer: the Western Australian experience.\",\"authors\":\"Dwayne T S Chang, Alarick Picardo\",\"doi\":\"10.14440/bladder.2020.814\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To determine the rate of residual disease and under-staging after primary transurethral resection (TUR) of bladder tumors (TURBT) in tertiary hospitals in Western Australia.</p><p><strong>Methods: </strong>A retrospective study was performed evaluating all patients with TaHG (stage Ta, high-grade), T1LG (stage T1, low-grade) or T1HG (stage T1, high-grade) bladder cancer on primary TURBT conducted between January 1, 2012 and December 31, 2017 at the four largest metropolitan public hospitals in Western Australia. Only patients who underwent repeat resection within 3 months from initial resection were included. Those with previous history of bladder cancer, incomplete follow-up data and visibly incomplete initial resection were excluded. Baseline patient demographics, macroscopic clearance at initial resection, and disease data at initial and repeat resections were recorded.</p><p><strong>Results: </strong>Sixty-seven patients with a median age of 71 years were included in this study. At initial resection, T1HG was the most common disease stage (64.2%) and detrusor muscle was present in 82.1% of initial resections. At repeat resection, 41.8% of cases had residual disease. The rate of upstaging to muscle-invasive bladder cancer was 3.0%. Patients treated by operators with five or less years of formal training did not have a significantly different rate of residual disease from patients treated by operators with more than five years of experience.</p><p><strong>Conclusions: </strong>Repeat TUR should remain an essential practice due to high rates of residual disease and a small risk of tumor under-staging. The presence of detrusor muscle and macroscopic clearance should not be used as surrogates for adequacy of resection or consideration of avoiding a repeat TUR, even for TaHG disease.</p>\",\"PeriodicalId\":72421,\"journal\":{\"name\":\"Bladder (San Francisco, Calif.)\",\"volume\":\"7 2\",\"pages\":\"e42\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-04-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/16/d1/bladder-7-2-e42.PMC7401982.pdf\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Bladder (San Francisco, Calif.)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14440/bladder.2020.814\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Bladder (San Francisco, Calif.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14440/bladder.2020.814","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Repeat transurethral resection is still an essential tool in treating non-muscle invasive bladder cancer: the Western Australian experience.
Objectives: To determine the rate of residual disease and under-staging after primary transurethral resection (TUR) of bladder tumors (TURBT) in tertiary hospitals in Western Australia.
Methods: A retrospective study was performed evaluating all patients with TaHG (stage Ta, high-grade), T1LG (stage T1, low-grade) or T1HG (stage T1, high-grade) bladder cancer on primary TURBT conducted between January 1, 2012 and December 31, 2017 at the four largest metropolitan public hospitals in Western Australia. Only patients who underwent repeat resection within 3 months from initial resection were included. Those with previous history of bladder cancer, incomplete follow-up data and visibly incomplete initial resection were excluded. Baseline patient demographics, macroscopic clearance at initial resection, and disease data at initial and repeat resections were recorded.
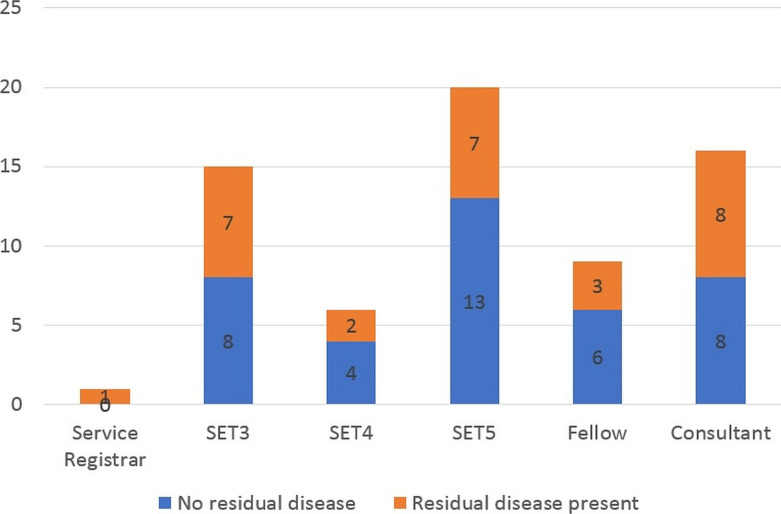
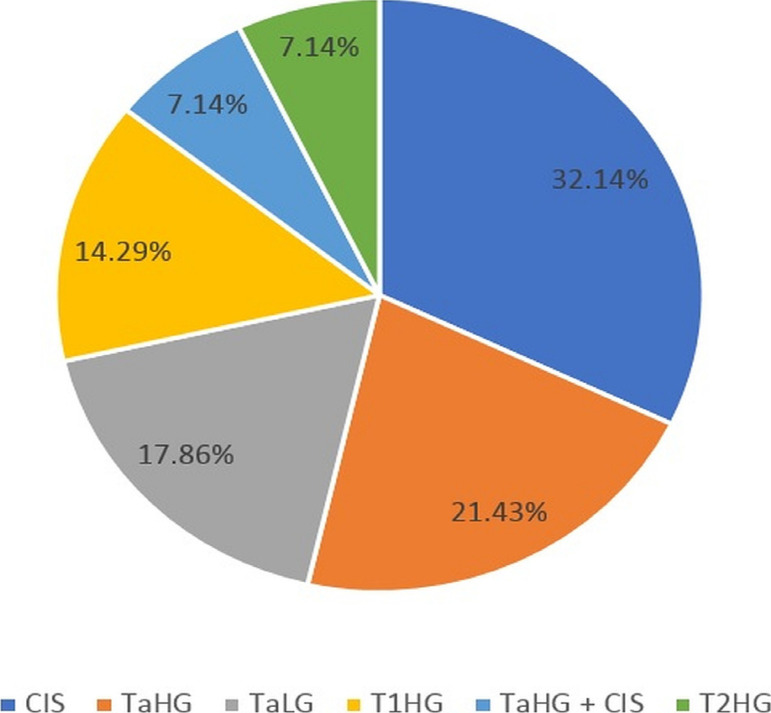
Results: Sixty-seven patients with a median age of 71 years were included in this study. At initial resection, T1HG was the most common disease stage (64.2%) and detrusor muscle was present in 82.1% of initial resections. At repeat resection, 41.8% of cases had residual disease. The rate of upstaging to muscle-invasive bladder cancer was 3.0%. Patients treated by operators with five or less years of formal training did not have a significantly different rate of residual disease from patients treated by operators with more than five years of experience.
Conclusions: Repeat TUR should remain an essential practice due to high rates of residual disease and a small risk of tumor under-staging. The presence of detrusor muscle and macroscopic clearance should not be used as surrogates for adequacy of resection or consideration of avoiding a repeat TUR, even for TaHG disease.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
