{"title":"SOFA评分预测静脉体外膜氧合成人心源性休克死亡率的有效性。","authors":"Mohamed Laimoud, Mosleh Alanazi","doi":"10.1155/2020/3129864","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Venoarterial ECMO is increasingly used in resuscitation of adult patients with cardiogenic shock with variable mortality reports worldwide. Our objectives were to study the variables associated with hospital mortality in adult patients supported with VA-ECMO and to determine the validity of repeated assessments of those patients by the Sequential Organ Failure Assessment (SOFA) score for prediction of hospital mortality. We retrospectively studied adult patients admitted to the cardiac surgical critical care unit with cardiogenic shock supported with VA-ECMO from January 2015 to August 2019 in our tertiary care hospital.</p><p><strong>Results: </strong>One hundred and six patients supported with VA-ECMO were included in our study with in-hospital mortality of 56.6%. The mean age of studied patients was 40.2 ± 14.4 years, and the patients were mostly males (69.8%) with a mean BMI of 26.5 ± 7 without statistically significant differences between survivors and nonsurvivors. Presence of CKD, chronic atrial fibrillation, and cardiac surgeries was significantly more frequent in the nonsurvivors group. The nonsurvivors had more frequent AKI (<i>p</i> < 0.001), more haemodialysis use (<i>p</i> < 0.001), more gastrointestinal bleeding (<i>p</i> = 0.039), more ICH (<i>p</i> = 0.006), and fewer ICU days (<i>p</i> = 0.002) compared to the survivors group. The mean peak blood lactate level was 11 ± 3 vs 16.7 ± 3.3, <i>p</i> < 0.001, and the mean lactate level after 24 hours of ECMO initiation was 2.2 ± 0.9 vs 7.9 ± 5.7, <i>p</i> < 0.001, in the survivors and nonsurvivors, respectively. Initial SOFA score ≥13 measured upon ICU admission had a 85% sensitivity and 73.9% specificity for predicting hospital mortality [AUROC = 0.862, 95% CI: 0.791-0.932; <i>p</i> < 0.001] with 81% PPV, 79.1% NPV, and 80.2% accuracy while SOFA score ≥13 at day 3 had 100% sensitivity and 91.3% specificity for predicting mortality with 93.8% PPV, 100% NPV, and 96.2% accuracy [AUROC = 0.995, 95% CI: 0.986-1; <i>p</i> < 0.001]. The ∆1 SOFA (3-1) ≥2 had 95% sensitivity and 93.5% specificity for predicting hospital mortality [AUROC = 0.958, 95% CI: 0.913-1; <i>p</i> < 0.001] with 95% PPV, 93.5% NPV, and 94.3% accuracy. SOFA score ≥15 at day 5 had 98% sensitivity and 100% specificity for predicting mortality with 99% accuracy [AUROC = 0.994, 95% CI: 0.982-1; <i>p</i> < 0.001]. The ∆2 SOFA (5-1) ≥2 had 90% sensitivity and 97.8% specificity for predicting hospital mortality [AUROC = 0.958, 95% CI: 0.909-1; <i>p</i> < 0.001] with 97.8% PPV, 90% NPV, and 94.8% accuracy. Multivariable regression analysis revealed that increasing ∆1 SOFA score (OR = 2.506, 95% CI: 1.681-3.735, <i>p</i> < 0.001) and increasing blood lactate level (OR = 1.388, 95% CI: 1.015-1.898, <i>p</i> = 0.04) were significantly associated with hospital mortality after VA-ECMO support for adults with cardiogenic shock.</p><p><strong>Conclusion: </strong>The use of VA-ECMO in adult patients with cardiogenic shock is still associated with high mortality. Serial evaluation of those patients with SOFA score during the first few days of ECMO support is a good predictor of hospital mortality. Increase in SOFA score after 48 hours and hyperlactataemia are significantly associated with increased hospital mortality.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2020 ","pages":"3129864"},"PeriodicalIF":1.8000,"publicationDate":"2020-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/3129864","citationCount":"17","resultStr":"{\"title\":\"The Validity of SOFA Score to Predict Mortality in Adult Patients with Cardiogenic Shock on Venoarterial Extracorporeal Membrane Oxygenation.\",\"authors\":\"Mohamed Laimoud, Mosleh Alanazi\",\"doi\":\"10.1155/2020/3129864\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Venoarterial ECMO is increasingly used in resuscitation of adult patients with cardiogenic shock with variable mortality reports worldwide. Our objectives were to study the variables associated with hospital mortality in adult patients supported with VA-ECMO and to determine the validity of repeated assessments of those patients by the Sequential Organ Failure Assessment (SOFA) score for prediction of hospital mortality. We retrospectively studied adult patients admitted to the cardiac surgical critical care unit with cardiogenic shock supported with VA-ECMO from January 2015 to August 2019 in our tertiary care hospital.</p><p><strong>Results: </strong>One hundred and six patients supported with VA-ECMO were included in our study with in-hospital mortality of 56.6%. The mean age of studied patients was 40.2 ± 14.4 years, and the patients were mostly males (69.8%) with a mean BMI of 26.5 ± 7 without statistically significant differences between survivors and nonsurvivors. Presence of CKD, chronic atrial fibrillation, and cardiac surgeries was significantly more frequent in the nonsurvivors group. The nonsurvivors had more frequent AKI (<i>p</i> < 0.001), more haemodialysis use (<i>p</i> < 0.001), more gastrointestinal bleeding (<i>p</i> = 0.039), more ICH (<i>p</i> = 0.006), and fewer ICU days (<i>p</i> = 0.002) compared to the survivors group. The mean peak blood lactate level was 11 ± 3 vs 16.7 ± 3.3, <i>p</i> < 0.001, and the mean lactate level after 24 hours of ECMO initiation was 2.2 ± 0.9 vs 7.9 ± 5.7, <i>p</i> < 0.001, in the survivors and nonsurvivors, respectively. Initial SOFA score ≥13 measured upon ICU admission had a 85% sensitivity and 73.9% specificity for predicting hospital mortality [AUROC = 0.862, 95% CI: 0.791-0.932; <i>p</i> < 0.001] with 81% PPV, 79.1% NPV, and 80.2% accuracy while SOFA score ≥13 at day 3 had 100% sensitivity and 91.3% specificity for predicting mortality with 93.8% PPV, 100% NPV, and 96.2% accuracy [AUROC = 0.995, 95% CI: 0.986-1; <i>p</i> < 0.001]. The ∆1 SOFA (3-1) ≥2 had 95% sensitivity and 93.5% specificity for predicting hospital mortality [AUROC = 0.958, 95% CI: 0.913-1; <i>p</i> < 0.001] with 95% PPV, 93.5% NPV, and 94.3% accuracy. SOFA score ≥15 at day 5 had 98% sensitivity and 100% specificity for predicting mortality with 99% accuracy [AUROC = 0.994, 95% CI: 0.982-1; <i>p</i> < 0.001]. The ∆2 SOFA (5-1) ≥2 had 90% sensitivity and 97.8% specificity for predicting hospital mortality [AUROC = 0.958, 95% CI: 0.909-1; <i>p</i> < 0.001] with 97.8% PPV, 90% NPV, and 94.8% accuracy. Multivariable regression analysis revealed that increasing ∆1 SOFA score (OR = 2.506, 95% CI: 1.681-3.735, <i>p</i> < 0.001) and increasing blood lactate level (OR = 1.388, 95% CI: 1.015-1.898, <i>p</i> = 0.04) were significantly associated with hospital mortality after VA-ECMO support for adults with cardiogenic shock.</p><p><strong>Conclusion: </strong>The use of VA-ECMO in adult patients with cardiogenic shock is still associated with high mortality. Serial evaluation of those patients with SOFA score during the first few days of ECMO support is a good predictor of hospital mortality. Increase in SOFA score after 48 hours and hyperlactataemia are significantly associated with increased hospital mortality.</p>\",\"PeriodicalId\":46583,\"journal\":{\"name\":\"Critical Care Research and Practice\",\"volume\":\"2020 \",\"pages\":\"3129864\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2020-09-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2020/3129864\",\"citationCount\":\"17\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2020/3129864\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/3129864","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
The Validity of SOFA Score to Predict Mortality in Adult Patients with Cardiogenic Shock on Venoarterial Extracorporeal Membrane Oxygenation.
Background: Venoarterial ECMO is increasingly used in resuscitation of adult patients with cardiogenic shock with variable mortality reports worldwide. Our objectives were to study the variables associated with hospital mortality in adult patients supported with VA-ECMO and to determine the validity of repeated assessments of those patients by the Sequential Organ Failure Assessment (SOFA) score for prediction of hospital mortality. We retrospectively studied adult patients admitted to the cardiac surgical critical care unit with cardiogenic shock supported with VA-ECMO from January 2015 to August 2019 in our tertiary care hospital.
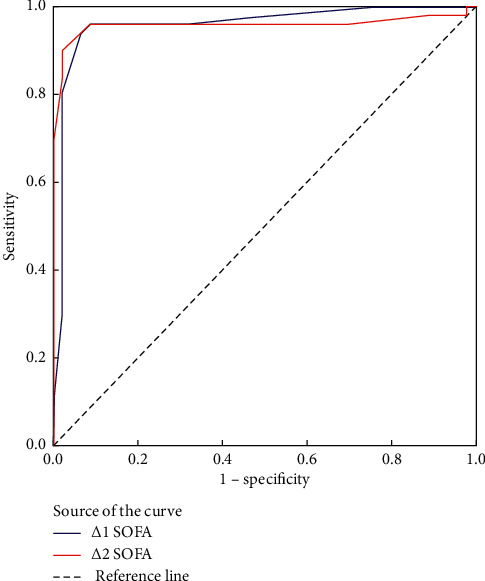
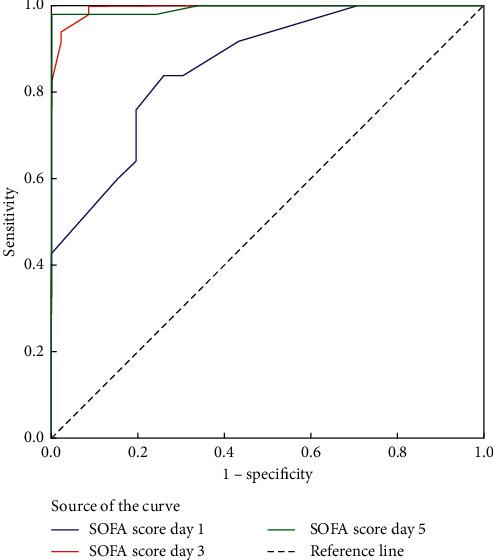
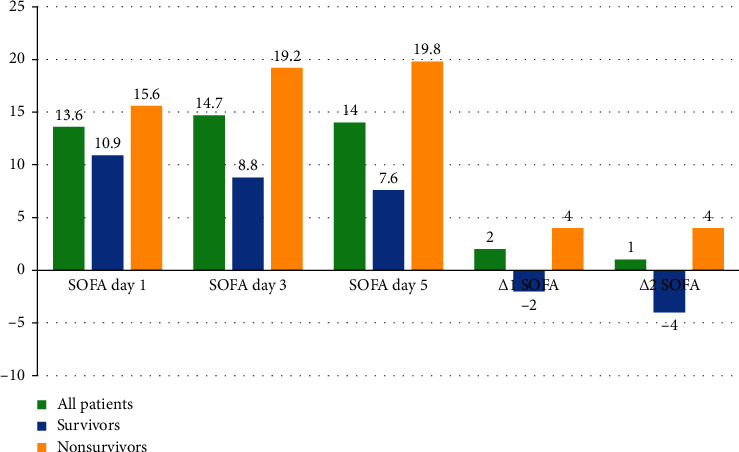
Results: One hundred and six patients supported with VA-ECMO were included in our study with in-hospital mortality of 56.6%. The mean age of studied patients was 40.2 ± 14.4 years, and the patients were mostly males (69.8%) with a mean BMI of 26.5 ± 7 without statistically significant differences between survivors and nonsurvivors. Presence of CKD, chronic atrial fibrillation, and cardiac surgeries was significantly more frequent in the nonsurvivors group. The nonsurvivors had more frequent AKI (p < 0.001), more haemodialysis use (p < 0.001), more gastrointestinal bleeding (p = 0.039), more ICH (p = 0.006), and fewer ICU days (p = 0.002) compared to the survivors group. The mean peak blood lactate level was 11 ± 3 vs 16.7 ± 3.3, p < 0.001, and the mean lactate level after 24 hours of ECMO initiation was 2.2 ± 0.9 vs 7.9 ± 5.7, p < 0.001, in the survivors and nonsurvivors, respectively. Initial SOFA score ≥13 measured upon ICU admission had a 85% sensitivity and 73.9% specificity for predicting hospital mortality [AUROC = 0.862, 95% CI: 0.791-0.932; p < 0.001] with 81% PPV, 79.1% NPV, and 80.2% accuracy while SOFA score ≥13 at day 3 had 100% sensitivity and 91.3% specificity for predicting mortality with 93.8% PPV, 100% NPV, and 96.2% accuracy [AUROC = 0.995, 95% CI: 0.986-1; p < 0.001]. The ∆1 SOFA (3-1) ≥2 had 95% sensitivity and 93.5% specificity for predicting hospital mortality [AUROC = 0.958, 95% CI: 0.913-1; p < 0.001] with 95% PPV, 93.5% NPV, and 94.3% accuracy. SOFA score ≥15 at day 5 had 98% sensitivity and 100% specificity for predicting mortality with 99% accuracy [AUROC = 0.994, 95% CI: 0.982-1; p < 0.001]. The ∆2 SOFA (5-1) ≥2 had 90% sensitivity and 97.8% specificity for predicting hospital mortality [AUROC = 0.958, 95% CI: 0.909-1; p < 0.001] with 97.8% PPV, 90% NPV, and 94.8% accuracy. Multivariable regression analysis revealed that increasing ∆1 SOFA score (OR = 2.506, 95% CI: 1.681-3.735, p < 0.001) and increasing blood lactate level (OR = 1.388, 95% CI: 1.015-1.898, p = 0.04) were significantly associated with hospital mortality after VA-ECMO support for adults with cardiogenic shock.
Conclusion: The use of VA-ECMO in adult patients with cardiogenic shock is still associated with high mortality. Serial evaluation of those patients with SOFA score during the first few days of ECMO support is a good predictor of hospital mortality. Increase in SOFA score after 48 hours and hyperlactataemia are significantly associated with increased hospital mortality.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
