Hunter K Holt, Shalini Kulasingam, Erinn C Sanstead, Fernando Alarid-Escudero, Karen Smith-McCune, Steven E Gregorich, Michael J Silverberg, Megan J Huchko, Miriam Kuppermann, George F Sawaya
{"title":"讨论子宫颈癌筛查方案:指导患者和提供者之间对话的结果。","authors":"Hunter K Holt, Shalini Kulasingam, Erinn C Sanstead, Fernando Alarid-Escudero, Karen Smith-McCune, Steven E Gregorich, Michael J Silverberg, Megan J Huchko, Miriam Kuppermann, George F Sawaya","doi":"10.1177/2381468320952409","DOIUrl":null,"url":null,"abstract":"<p><p><b>Purpose.</b> In 2018, the US Preventive Services Task Force (USPSTF) endorsed three strategies for cervical cancer screening in women ages 30 to 65: cytology every 3 years, testing for high-risk types of human papillomavirus (hrHPV) every 5 years, and cytology plus hrHPV testing (co-testing) every 5 years. It further recommended that women discuss with health care providers which testing strategy is best for them. To inform such discussions, we used decision analysis to estimate outcomes of screening strategies recommended for women at age 30. <b>Methods.</b> We constructed a Markov decision model using estimates of the natural history of HPV and cervical neoplasia. We evaluated the three USPSTF-endorsed strategies, hrHPV testing every 3 years and no screening. Outcomes included colposcopies with biopsy, false-positive testing (a colposcopy in which no cervical intraepithelial neoplasia grade 2 or worse was found), treatments, cancers, and cancer mortality expressed per 10,000 women over a shorter-than-lifetime horizon (15-year). <b>Results.</b> All strategies resulted in substantially lower cancer and cancer death rates compared with no screening. Strategies with the lowest likelihood of cancer and cancer death generally had higher likelihood of colposcopy and false-positive testing. <b>Conclusions.</b> The screening strategies we evaluated involved tradeoffs in terms of benefits and harms. Because individual women may place different weights on these projected outcomes, the optimal choice for each woman may best be discerned through shared decision making.</p>","PeriodicalId":36567,"journal":{"name":"MDM Policy and Practice","volume":"5 2","pages":"2381468320952409"},"PeriodicalIF":1.7000,"publicationDate":"2020-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/30/a4/10.1177_2381468320952409.PMC7440733.pdf","citationCount":"0","resultStr":"{\"title\":\"Discussing Cervical Cancer Screening Options: Outcomes to Guide Conversations Between Patients and Providers.\",\"authors\":\"Hunter K Holt, Shalini Kulasingam, Erinn C Sanstead, Fernando Alarid-Escudero, Karen Smith-McCune, Steven E Gregorich, Michael J Silverberg, Megan J Huchko, Miriam Kuppermann, George F Sawaya\",\"doi\":\"10.1177/2381468320952409\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Purpose.</b> In 2018, the US Preventive Services Task Force (USPSTF) endorsed three strategies for cervical cancer screening in women ages 30 to 65: cytology every 3 years, testing for high-risk types of human papillomavirus (hrHPV) every 5 years, and cytology plus hrHPV testing (co-testing) every 5 years. It further recommended that women discuss with health care providers which testing strategy is best for them. To inform such discussions, we used decision analysis to estimate outcomes of screening strategies recommended for women at age 30. <b>Methods.</b> We constructed a Markov decision model using estimates of the natural history of HPV and cervical neoplasia. We evaluated the three USPSTF-endorsed strategies, hrHPV testing every 3 years and no screening. Outcomes included colposcopies with biopsy, false-positive testing (a colposcopy in which no cervical intraepithelial neoplasia grade 2 or worse was found), treatments, cancers, and cancer mortality expressed per 10,000 women over a shorter-than-lifetime horizon (15-year). <b>Results.</b> All strategies resulted in substantially lower cancer and cancer death rates compared with no screening. Strategies with the lowest likelihood of cancer and cancer death generally had higher likelihood of colposcopy and false-positive testing. <b>Conclusions.</b> The screening strategies we evaluated involved tradeoffs in terms of benefits and harms. Because individual women may place different weights on these projected outcomes, the optimal choice for each woman may best be discerned through shared decision making.</p>\",\"PeriodicalId\":36567,\"journal\":{\"name\":\"MDM Policy and Practice\",\"volume\":\"5 2\",\"pages\":\"2381468320952409\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2020-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/30/a4/10.1177_2381468320952409.PMC7440733.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"MDM Policy and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/2381468320952409\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"HEALTH CARE SCIENCES & SERVICES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"MDM Policy and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2381468320952409","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
Discussing Cervical Cancer Screening Options: Outcomes to Guide Conversations Between Patients and Providers.
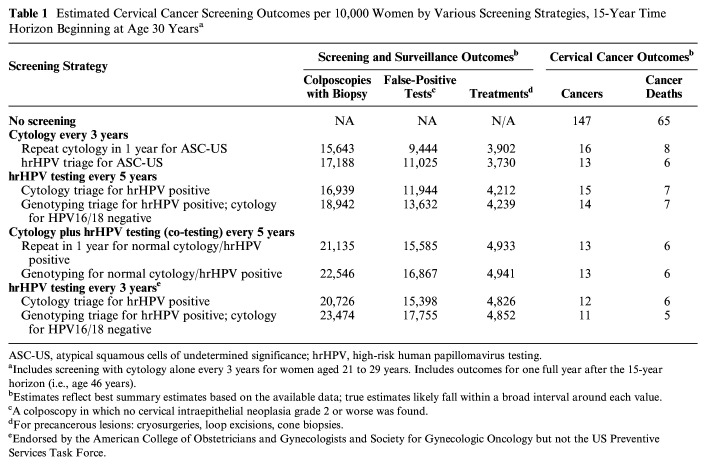
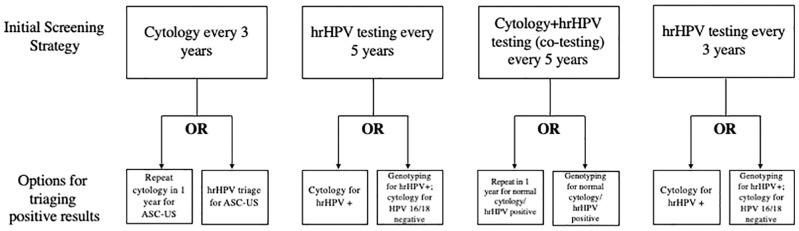
Purpose. In 2018, the US Preventive Services Task Force (USPSTF) endorsed three strategies for cervical cancer screening in women ages 30 to 65: cytology every 3 years, testing for high-risk types of human papillomavirus (hrHPV) every 5 years, and cytology plus hrHPV testing (co-testing) every 5 years. It further recommended that women discuss with health care providers which testing strategy is best for them. To inform such discussions, we used decision analysis to estimate outcomes of screening strategies recommended for women at age 30. Methods. We constructed a Markov decision model using estimates of the natural history of HPV and cervical neoplasia. We evaluated the three USPSTF-endorsed strategies, hrHPV testing every 3 years and no screening. Outcomes included colposcopies with biopsy, false-positive testing (a colposcopy in which no cervical intraepithelial neoplasia grade 2 or worse was found), treatments, cancers, and cancer mortality expressed per 10,000 women over a shorter-than-lifetime horizon (15-year). Results. All strategies resulted in substantially lower cancer and cancer death rates compared with no screening. Strategies with the lowest likelihood of cancer and cancer death generally had higher likelihood of colposcopy and false-positive testing. Conclusions. The screening strategies we evaluated involved tradeoffs in terms of benefits and harms. Because individual women may place different weights on these projected outcomes, the optimal choice for each woman may best be discerned through shared decision making.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
