Ratna Acharya, Xu Zeng, William L Clapp, Kiran Upadhyay
{"title":"肝硬化Wilson病IgA血管炎伴肾炎:两者有关联吗?","authors":"Ratna Acharya, Xu Zeng, William L Clapp, Kiran Upadhyay","doi":"10.5414/CNCS110268","DOIUrl":null,"url":null,"abstract":"Introduction: IgA vasculitis (IgA-V) predominantly involves skin, gastrointestinal (GI) tract, joints, and kidneys. Wilson disease (WD) is a hepatolenticular degenerative disease caused by ATP7B gene mutation. Case report: Here we describe an unusual association of IgA-V with nephritis (IgA-VN) in an 11-year-old child with WD. He presented with palpable purpura without arthritis and GI involvement. Renal function was normal. Urinalysis showed microscopic hematuria and tubular proteinuria. Evaluation showed transaminitis, hypoalbuminemia, IgA hyperglobulinemia, and coagulation abnormalities. Serum ceruloplasmin and copper were low and 24-hour urine copper was extremely elevated. Liver biopsy showed stage IV cirrhosis with increased quantitative liver copper content. Skin and renal biopsy showed IgA-positive leukocytoclastic vasculitis and mesangial hyperplasia with IgA deposition, respectively. Quantitative renal copper content was normal. Homozygous pathogenic variant c.3207C>A (p.His1069Gln) of ATP7B was detected. There were no Kayser-Fleischer rings in the eyes, and neuropsychiatric examination was normal. Treatment with zinc and trientine led to normalization of hepatic function and serum IgA level with resolution of the rash and maintenance of renal function. Conclusion: Defective hepatic processing and/or clearance of IgA/IgA immune complexes probably led to the IgA-mediated skin and renal injury. Further such reports will help augment our understanding on the pathophysiology of IgA-VN in WD.","PeriodicalId":10398,"journal":{"name":"Clinical Nephrology. Case Studies","volume":"8 ","pages":"80-84"},"PeriodicalIF":0.0000,"publicationDate":"2020-10-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7552349/pdf/","citationCount":"4","resultStr":"{\"title\":\"IgA vasculitis with nephritis in cirrhotic Wilson disease: Is there an association?\",\"authors\":\"Ratna Acharya, Xu Zeng, William L Clapp, Kiran Upadhyay\",\"doi\":\"10.5414/CNCS110268\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Introduction: IgA vasculitis (IgA-V) predominantly involves skin, gastrointestinal (GI) tract, joints, and kidneys. Wilson disease (WD) is a hepatolenticular degenerative disease caused by ATP7B gene mutation. Case report: Here we describe an unusual association of IgA-V with nephritis (IgA-VN) in an 11-year-old child with WD. He presented with palpable purpura without arthritis and GI involvement. Renal function was normal. Urinalysis showed microscopic hematuria and tubular proteinuria. Evaluation showed transaminitis, hypoalbuminemia, IgA hyperglobulinemia, and coagulation abnormalities. Serum ceruloplasmin and copper were low and 24-hour urine copper was extremely elevated. Liver biopsy showed stage IV cirrhosis with increased quantitative liver copper content. Skin and renal biopsy showed IgA-positive leukocytoclastic vasculitis and mesangial hyperplasia with IgA deposition, respectively. Quantitative renal copper content was normal. Homozygous pathogenic variant c.3207C>A (p.His1069Gln) of ATP7B was detected. There were no Kayser-Fleischer rings in the eyes, and neuropsychiatric examination was normal. Treatment with zinc and trientine led to normalization of hepatic function and serum IgA level with resolution of the rash and maintenance of renal function. Conclusion: Defective hepatic processing and/or clearance of IgA/IgA immune complexes probably led to the IgA-mediated skin and renal injury. Further such reports will help augment our understanding on the pathophysiology of IgA-VN in WD.\",\"PeriodicalId\":10398,\"journal\":{\"name\":\"Clinical Nephrology. Case Studies\",\"volume\":\"8 \",\"pages\":\"80-84\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-10-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7552349/pdf/\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Nephrology. Case Studies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5414/CNCS110268\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nephrology. Case Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS110268","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
IgA vasculitis with nephritis in cirrhotic Wilson disease: Is there an association?
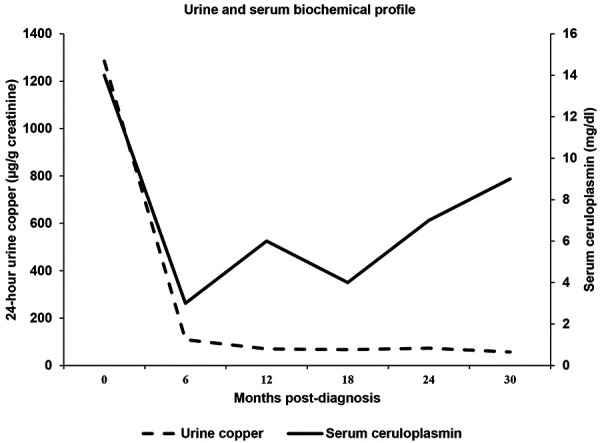
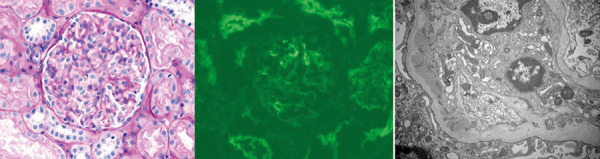
Introduction: IgA vasculitis (IgA-V) predominantly involves skin, gastrointestinal (GI) tract, joints, and kidneys. Wilson disease (WD) is a hepatolenticular degenerative disease caused by ATP7B gene mutation. Case report: Here we describe an unusual association of IgA-V with nephritis (IgA-VN) in an 11-year-old child with WD. He presented with palpable purpura without arthritis and GI involvement. Renal function was normal. Urinalysis showed microscopic hematuria and tubular proteinuria. Evaluation showed transaminitis, hypoalbuminemia, IgA hyperglobulinemia, and coagulation abnormalities. Serum ceruloplasmin and copper were low and 24-hour urine copper was extremely elevated. Liver biopsy showed stage IV cirrhosis with increased quantitative liver copper content. Skin and renal biopsy showed IgA-positive leukocytoclastic vasculitis and mesangial hyperplasia with IgA deposition, respectively. Quantitative renal copper content was normal. Homozygous pathogenic variant c.3207C>A (p.His1069Gln) of ATP7B was detected. There were no Kayser-Fleischer rings in the eyes, and neuropsychiatric examination was normal. Treatment with zinc and trientine led to normalization of hepatic function and serum IgA level with resolution of the rash and maintenance of renal function. Conclusion: Defective hepatic processing and/or clearance of IgA/IgA immune complexes probably led to the IgA-mediated skin and renal injury. Further such reports will help augment our understanding on the pathophysiology of IgA-VN in WD.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
