{"title":"12 周及以上流产的医疗方案:系统回顾和荟萃分析","authors":"Katherine Whitehouse , Ashley Brant , Marita Sporstol Fonhus , Antonella Lavelanet , Bela Ganatra","doi":"10.1016/j.conx.2020.100037","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Mifepristone and misoprostol are recommended for second-trimester medical abortion, but consensus is unclear on the ideal regimen.</p></div><div><h3>Objectives</h3><p>The objectives were to systematically review randomized controlled trials (RCTs) investigating efficacy, safety and satisfaction of medical abortion at ≥<!--> <!-->12 weeks' gestation.</p></div><div><h3>Data sources</h3><p>We searched PubMed, Popline, Embase, Global Index Medicus, Cochrane Controlled Register of Trials and International Clinical Trials Registry Platform from January 2008 to May 2017.</p></div><div><h3>Study eligibility, participants and interventions</h3><p>We included RCTs on medical abortion at ≥<!--> <!-->12 weeks' gestation using mifepristone and/or misoprostol. We excluded studies with spontaneous abortion, fetal demise and mechanical cervical ripening and those not reporting ongoing pregnancy (OP).</p></div><div><h3>Study appraisal and synthesis methods</h3><p>After extracting prespecified data and assessing risk of bias in accordance with the Cochrane handbook, we used Revman5 software to combine data and GRADE to assess certainty of evidence.</p></div><div><h3>Results</h3><p>We included 43 of the 1894 references identified. Combination mifepristone–misoprostol had lower rates of OP [risk ratio (RR) 0.12, 95% confidence interval (CI) 0.04–0.35] vs. misoprostol only. A 24-h interval between mifepristone and misoprostol had lower OP rate at 24 h than simultaneous dosing (RR 3.13, 95% CI 1.23–7.94). Every 3-h dosing had lower OP rate at 48 h (RR 0.39, 95% CI 0.17–0.88).</p></div><div><h3>Limitations</h3><p>Direct comparisons of buccal misoprostol to sublingual or vaginal routes after mifepristone were limited. Evidence from clinical trials on how to best manage women with prior uterine incisions was lacking.</p></div><div><h3>Conclusion</h3><p>Our analysis supports the use of mifepristone 200 mg 1 to 2 days before misoprostol 400 mcg vaginally every 3 h at ≥<!--> <!-->12 weeks' gestation.</p></div><div><h3>Implications</h3><p>Where available, providers should use mifepristone plus misoprostol for second-trimester medical abortion. Vaginal misoprostol appears to be most efficacious with fewest side effects, but sublingual and buccal routes are also acceptable.</p></div>","PeriodicalId":10655,"journal":{"name":"Contraception: X","volume":"2 ","pages":"Article 100037"},"PeriodicalIF":0.0000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.conx.2020.100037","citationCount":"8","resultStr":"{\"title\":\"Medical regimens for abortion at 12 weeks and above: a systematic review and meta-analysis\",\"authors\":\"Katherine Whitehouse , Ashley Brant , Marita Sporstol Fonhus , Antonella Lavelanet , Bela Ganatra\",\"doi\":\"10.1016/j.conx.2020.100037\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Mifepristone and misoprostol are recommended for second-trimester medical abortion, but consensus is unclear on the ideal regimen.</p></div><div><h3>Objectives</h3><p>The objectives were to systematically review randomized controlled trials (RCTs) investigating efficacy, safety and satisfaction of medical abortion at ≥<!--> <!-->12 weeks' gestation.</p></div><div><h3>Data sources</h3><p>We searched PubMed, Popline, Embase, Global Index Medicus, Cochrane Controlled Register of Trials and International Clinical Trials Registry Platform from January 2008 to May 2017.</p></div><div><h3>Study eligibility, participants and interventions</h3><p>We included RCTs on medical abortion at ≥<!--> <!-->12 weeks' gestation using mifepristone and/or misoprostol. We excluded studies with spontaneous abortion, fetal demise and mechanical cervical ripening and those not reporting ongoing pregnancy (OP).</p></div><div><h3>Study appraisal and synthesis methods</h3><p>After extracting prespecified data and assessing risk of bias in accordance with the Cochrane handbook, we used Revman5 software to combine data and GRADE to assess certainty of evidence.</p></div><div><h3>Results</h3><p>We included 43 of the 1894 references identified. Combination mifepristone–misoprostol had lower rates of OP [risk ratio (RR) 0.12, 95% confidence interval (CI) 0.04–0.35] vs. misoprostol only. A 24-h interval between mifepristone and misoprostol had lower OP rate at 24 h than simultaneous dosing (RR 3.13, 95% CI 1.23–7.94). Every 3-h dosing had lower OP rate at 48 h (RR 0.39, 95% CI 0.17–0.88).</p></div><div><h3>Limitations</h3><p>Direct comparisons of buccal misoprostol to sublingual or vaginal routes after mifepristone were limited. Evidence from clinical trials on how to best manage women with prior uterine incisions was lacking.</p></div><div><h3>Conclusion</h3><p>Our analysis supports the use of mifepristone 200 mg 1 to 2 days before misoprostol 400 mcg vaginally every 3 h at ≥<!--> <!-->12 weeks' gestation.</p></div><div><h3>Implications</h3><p>Where available, providers should use mifepristone plus misoprostol for second-trimester medical abortion. Vaginal misoprostol appears to be most efficacious with fewest side effects, but sublingual and buccal routes are also acceptable.</p></div>\",\"PeriodicalId\":10655,\"journal\":{\"name\":\"Contraception: X\",\"volume\":\"2 \",\"pages\":\"Article 100037\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1016/j.conx.2020.100037\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Contraception: X\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2590151620300204\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/8/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Contraception: X","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590151620300204","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/8/20 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 8
摘要
背景:米非司酮和米索前列醇被推荐用于中期妊娠药物流产,但对于理想方案的共识尚不明确。目的系统回顾研究妊娠≥12 周药物流产的疗效、安全性和满意度的随机对照试验(rct)。我们检索了2008年1月至2017年5月的PubMed、Popline、Embase、Global Index Medicus、Cochrane Controlled Register of Trials和国际临床试验注册平台。研究资格、参与者和干预措施我们纳入了妊娠≥12 周使用米非司酮和/或米索前列醇进行药物流产的随机对照试验。我们排除了自然流产、胎儿死亡、机械宫颈成熟和未报告妊娠的研究。研究评价和综合方法在提取预先指定的数据并根据Cochrane手册评估偏倚风险后,我们使用Revman5软件将数据和GRADE结合起来评估证据的确定性。结果纳入1894篇文献中的43篇。米非司酮-米索前列醇联合治疗的OP发生率较单用米索前列醇低[风险比(RR) 0.12, 95%可信区间(CI) 0.04-0.35]。米非司酮和米索前列醇之间间隔24 h,在24 h时的OP率低于同时给药(RR 3.13, 95% CI 1.23-7.94)。每给药3 h,在48 h时OP率降低(RR 0.39, 95% CI 0.17-0.88)。局限性:米非司酮后口腔米索前列醇与舌下或阴道途径的直接比较是有限的。缺乏关于如何最好地处理既往子宫切口妇女的临床试验证据。结论:我们的分析支持在妊娠≥12 周时,米非司酮200 mg先于米索前列醇400 mcg每3 h阴道使用1 - 2天。在可能的情况下,提供者应使用米非司酮加米索前列醇进行中期妊娠药物流产。阴道米索前列醇似乎是最有效的,副作用最少,但舌下和口腔途径也是可以接受的。
Medical regimens for abortion at 12 weeks and above: a systematic review and meta-analysis
Background
Mifepristone and misoprostol are recommended for second-trimester medical abortion, but consensus is unclear on the ideal regimen.
Objectives
The objectives were to systematically review randomized controlled trials (RCTs) investigating efficacy, safety and satisfaction of medical abortion at ≥ 12 weeks' gestation.
Data sources
We searched PubMed, Popline, Embase, Global Index Medicus, Cochrane Controlled Register of Trials and International Clinical Trials Registry Platform from January 2008 to May 2017.
Study eligibility, participants and interventions
We included RCTs on medical abortion at ≥ 12 weeks' gestation using mifepristone and/or misoprostol. We excluded studies with spontaneous abortion, fetal demise and mechanical cervical ripening and those not reporting ongoing pregnancy (OP).
Study appraisal and synthesis methods
After extracting prespecified data and assessing risk of bias in accordance with the Cochrane handbook, we used Revman5 software to combine data and GRADE to assess certainty of evidence.
Results
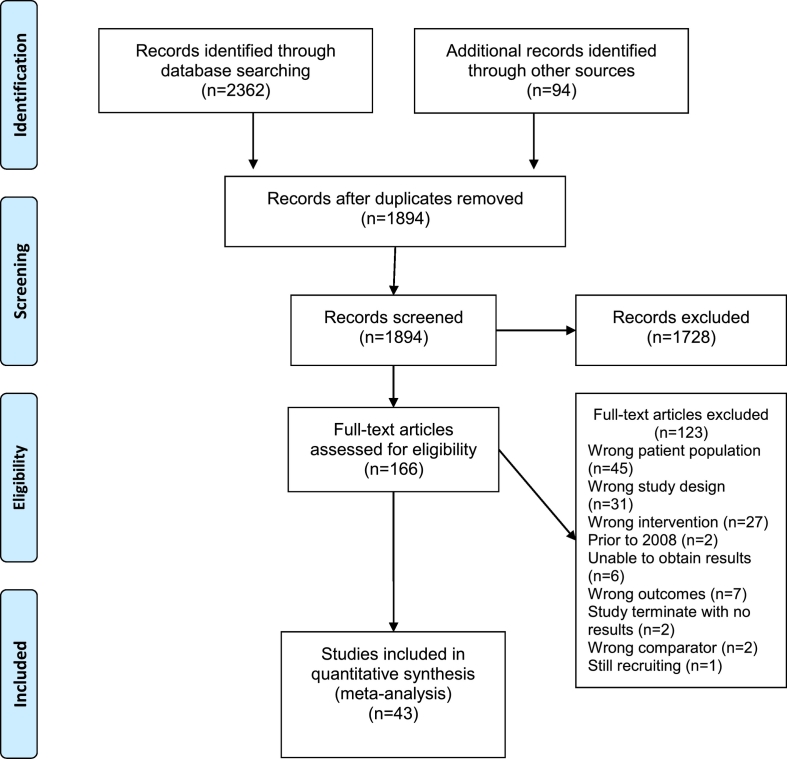
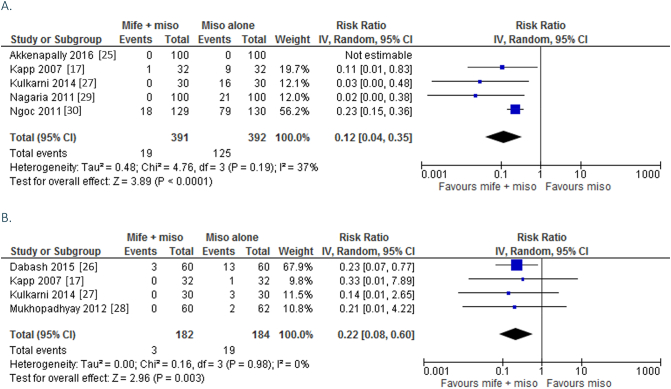
We included 43 of the 1894 references identified. Combination mifepristone–misoprostol had lower rates of OP [risk ratio (RR) 0.12, 95% confidence interval (CI) 0.04–0.35] vs. misoprostol only. A 24-h interval between mifepristone and misoprostol had lower OP rate at 24 h than simultaneous dosing (RR 3.13, 95% CI 1.23–7.94). Every 3-h dosing had lower OP rate at 48 h (RR 0.39, 95% CI 0.17–0.88).
Limitations
Direct comparisons of buccal misoprostol to sublingual or vaginal routes after mifepristone were limited. Evidence from clinical trials on how to best manage women with prior uterine incisions was lacking.
Conclusion
Our analysis supports the use of mifepristone 200 mg 1 to 2 days before misoprostol 400 mcg vaginally every 3 h at ≥ 12 weeks' gestation.
Implications
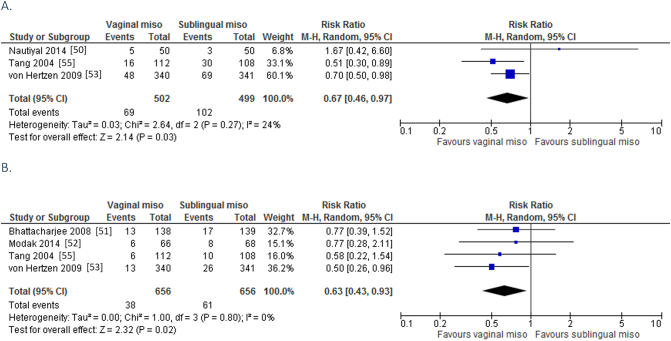
Where available, providers should use mifepristone plus misoprostol for second-trimester medical abortion. Vaginal misoprostol appears to be most efficacious with fewest side effects, but sublingual and buccal routes are also acceptable.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
