Anne Schoenmakers, Liesbeth Mieras, Teky Budiawan, Wim H van Brakel
{"title":"暴露后麻风病预防的现状:关于免疫和化学预防的描述性元分析。","authors":"Anne Schoenmakers, Liesbeth Mieras, Teky Budiawan, Wim H van Brakel","doi":"10.2147/RRTM.S190300","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Annually, over 200,000 people are diagnosed with leprosy, also called Hansen's disease. This number has been relatively stable over the past years. Progress has been made in the fields of chemoprophylaxis and immunoprophylaxis to prevent leprosy, with a primary focus on close contacts of patients. In this descriptive meta-analysis, we summarize the evidence and identify knowledge gaps regarding post-exposure prophylaxis against leprosy.</p><p><strong>Methods: </strong>A systematic literature search according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology was conducted by searching the medical scientific databases Cochrane, Embase, Pubmed/MEDLINE, Research Gate, Scopus and Web of Science on Jan. 22, 2020, using a combination of synonyms for index terms in four languages: \"leprosy\" and \"population\" or \"contacts\" and \"prevention\" or \"prophylaxis.\" Subsequently, Infolep.org and Google Scholar were searched and the \"snowball method\" was used to retrieve other potentially relevant literature. The found articles were screened for eligibility using predetermined inclusion and exclusion criteria.</p><p><strong>Results: </strong>After deduplication, 1,515 articles were screened, and 125 articles were included in this descriptive meta-analysis. Immunoprophylaxis by bacillus Calmette-Guérin (BCG) vaccination is known to provide protection against leprosy. The protection it offers is higher in household contacts of leprosy patients compared with the general population and is seen to decline over time. Contact follow-up screening is important in the first period after BCG administration, as a substantial number of new leprosy patients presents three months post-vaccination. Evidence for the benefit of re-vaccination is conflicting. The World Health Organization (WHO) included BCG in its Guidelines for the Diagnosis, Treatment and Prevention of Leprosy by stating that BCG at birth should be maintained in at least all leprosy high-burden regions. Literature shows that several vaccination interventions with other immunoprophylactic agents demonstrate similar or slightly less efficacy in leprosy risk reduction compared with BCG. However, most of these studies do not exclusively focus on post-exposure prophylaxis. Two vaccines are considered future candidates for leprosy prophylaxis: <i>Mycobacterium indicus pranii</i> (<i>MiP</i>) and LepVax. For chemoprophylaxis, trials were performed with dapsone/acedapsone, rifampicin, and ROM, a combination of rifampicin, ofloxacin, and minocycline. Single-dose rifampicin is favored as post-exposure prophylaxis, abbreviated as SDR-PEP. It demonstrated a protective effect of 57% in the first two years after administration to contacts of leprosy patients. It is inexpensive, and adverse events are rare. The risk of SDR-PEP inducing rifampicin resistance is considered negligible, but continuous monitoring in accordance with WHO policies should be encouraged. The integration of contact screening and SDR-PEP administration into different leprosy control programs was found to be feasible and well accepted. Since 2018, SDR-PEP is included in the WHO Guidelines for the Diagnosis, Treatment and Prevention of Leprosy.</p><p><strong>Conclusion: </strong>Progress has been made in the areas of chemoprophylaxis and immunoprophylaxis to prevent leprosy in contacts of patients. Investing in vaccine studies, like LepVax and <i>MiP,</i> and increasing harmonization between tuberculosis (TB) and leprosy research groups is important. SDR-PEP is promising as a chemoprophylactic agent, and further implementation should be promoted. More chemoprophylaxis research is needed on: enhanced medication regimens; interventions in varying (epidemiological) settings, including focal mass drug administration (fMDA); specific approaches per contact type; combinations with screening variations and field-friendly rapid tests, if available in the future; community and health staff education; ongoing antibiotic resistance surveillance; and administering chemoprophylaxis with SDR-PEP prior to BCG administration. Additionally, both leprosy prophylactic drug registration nationally and prophylactic drug availability globally at low or no cost are important for the implementation and further upscaling of preventive measures against leprosy, such as SDR-PEP and new vaccines.</p>","PeriodicalId":21138,"journal":{"name":"Research and Reports in Tropical Medicine","volume":"11 ","pages":"97-117"},"PeriodicalIF":4.5000,"publicationDate":"2020-10-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a6/02/rrtm-11-97.PMC7573302.pdf","citationCount":"0","resultStr":"{\"title\":\"The State of Affairs in Post-Exposure Leprosy Prevention: A Descriptive Meta-Analysis on Immuno- and Chemo-Prophylaxis.\",\"authors\":\"Anne Schoenmakers, Liesbeth Mieras, Teky Budiawan, Wim H van Brakel\",\"doi\":\"10.2147/RRTM.S190300\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>Annually, over 200,000 people are diagnosed with leprosy, also called Hansen's disease. This number has been relatively stable over the past years. Progress has been made in the fields of chemoprophylaxis and immunoprophylaxis to prevent leprosy, with a primary focus on close contacts of patients. In this descriptive meta-analysis, we summarize the evidence and identify knowledge gaps regarding post-exposure prophylaxis against leprosy.</p><p><strong>Methods: </strong>A systematic literature search according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology was conducted by searching the medical scientific databases Cochrane, Embase, Pubmed/MEDLINE, Research Gate, Scopus and Web of Science on Jan. 22, 2020, using a combination of synonyms for index terms in four languages: \\\"leprosy\\\" and \\\"population\\\" or \\\"contacts\\\" and \\\"prevention\\\" or \\\"prophylaxis.\\\" Subsequently, Infolep.org and Google Scholar were searched and the \\\"snowball method\\\" was used to retrieve other potentially relevant literature. The found articles were screened for eligibility using predetermined inclusion and exclusion criteria.</p><p><strong>Results: </strong>After deduplication, 1,515 articles were screened, and 125 articles were included in this descriptive meta-analysis. Immunoprophylaxis by bacillus Calmette-Guérin (BCG) vaccination is known to provide protection against leprosy. The protection it offers is higher in household contacts of leprosy patients compared with the general population and is seen to decline over time. Contact follow-up screening is important in the first period after BCG administration, as a substantial number of new leprosy patients presents three months post-vaccination. Evidence for the benefit of re-vaccination is conflicting. The World Health Organization (WHO) included BCG in its Guidelines for the Diagnosis, Treatment and Prevention of Leprosy by stating that BCG at birth should be maintained in at least all leprosy high-burden regions. Literature shows that several vaccination interventions with other immunoprophylactic agents demonstrate similar or slightly less efficacy in leprosy risk reduction compared with BCG. However, most of these studies do not exclusively focus on post-exposure prophylaxis. Two vaccines are considered future candidates for leprosy prophylaxis: <i>Mycobacterium indicus pranii</i> (<i>MiP</i>) and LepVax. For chemoprophylaxis, trials were performed with dapsone/acedapsone, rifampicin, and ROM, a combination of rifampicin, ofloxacin, and minocycline. Single-dose rifampicin is favored as post-exposure prophylaxis, abbreviated as SDR-PEP. It demonstrated a protective effect of 57% in the first two years after administration to contacts of leprosy patients. It is inexpensive, and adverse events are rare. The risk of SDR-PEP inducing rifampicin resistance is considered negligible, but continuous monitoring in accordance with WHO policies should be encouraged. The integration of contact screening and SDR-PEP administration into different leprosy control programs was found to be feasible and well accepted. Since 2018, SDR-PEP is included in the WHO Guidelines for the Diagnosis, Treatment and Prevention of Leprosy.</p><p><strong>Conclusion: </strong>Progress has been made in the areas of chemoprophylaxis and immunoprophylaxis to prevent leprosy in contacts of patients. Investing in vaccine studies, like LepVax and <i>MiP,</i> and increasing harmonization between tuberculosis (TB) and leprosy research groups is important. SDR-PEP is promising as a chemoprophylactic agent, and further implementation should be promoted. More chemoprophylaxis research is needed on: enhanced medication regimens; interventions in varying (epidemiological) settings, including focal mass drug administration (fMDA); specific approaches per contact type; combinations with screening variations and field-friendly rapid tests, if available in the future; community and health staff education; ongoing antibiotic resistance surveillance; and administering chemoprophylaxis with SDR-PEP prior to BCG administration. Additionally, both leprosy prophylactic drug registration nationally and prophylactic drug availability globally at low or no cost are important for the implementation and further upscaling of preventive measures against leprosy, such as SDR-PEP and new vaccines.</p>\",\"PeriodicalId\":21138,\"journal\":{\"name\":\"Research and Reports in Tropical Medicine\",\"volume\":\"11 \",\"pages\":\"97-117\"},\"PeriodicalIF\":4.5000,\"publicationDate\":\"2020-10-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a6/02/rrtm-11-97.PMC7573302.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Research and Reports in Tropical Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2147/RRTM.S190300\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Research and Reports in Tropical Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/RRTM.S190300","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
The State of Affairs in Post-Exposure Leprosy Prevention: A Descriptive Meta-Analysis on Immuno- and Chemo-Prophylaxis.
Objective: Annually, over 200,000 people are diagnosed with leprosy, also called Hansen's disease. This number has been relatively stable over the past years. Progress has been made in the fields of chemoprophylaxis and immunoprophylaxis to prevent leprosy, with a primary focus on close contacts of patients. In this descriptive meta-analysis, we summarize the evidence and identify knowledge gaps regarding post-exposure prophylaxis against leprosy.
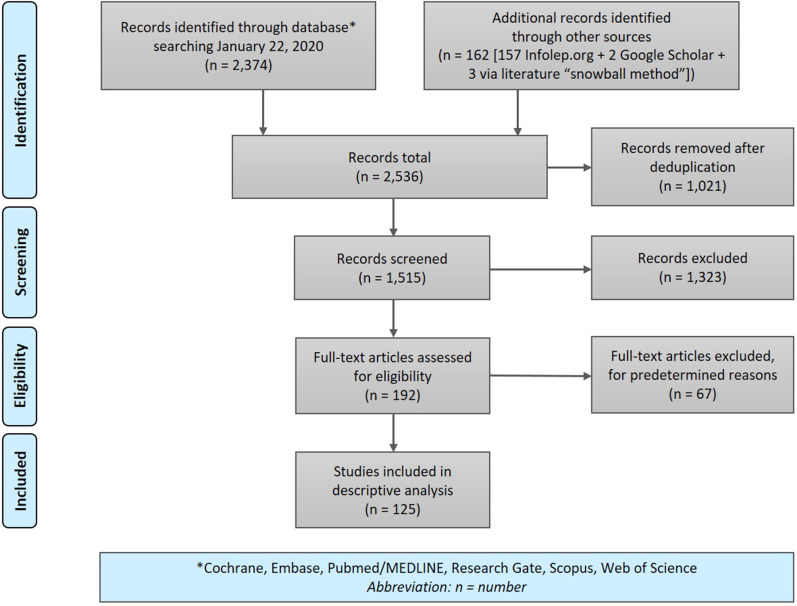
Methods: A systematic literature search according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) methodology was conducted by searching the medical scientific databases Cochrane, Embase, Pubmed/MEDLINE, Research Gate, Scopus and Web of Science on Jan. 22, 2020, using a combination of synonyms for index terms in four languages: "leprosy" and "population" or "contacts" and "prevention" or "prophylaxis." Subsequently, Infolep.org and Google Scholar were searched and the "snowball method" was used to retrieve other potentially relevant literature. The found articles were screened for eligibility using predetermined inclusion and exclusion criteria.
Results: After deduplication, 1,515 articles were screened, and 125 articles were included in this descriptive meta-analysis. Immunoprophylaxis by bacillus Calmette-Guérin (BCG) vaccination is known to provide protection against leprosy. The protection it offers is higher in household contacts of leprosy patients compared with the general population and is seen to decline over time. Contact follow-up screening is important in the first period after BCG administration, as a substantial number of new leprosy patients presents three months post-vaccination. Evidence for the benefit of re-vaccination is conflicting. The World Health Organization (WHO) included BCG in its Guidelines for the Diagnosis, Treatment and Prevention of Leprosy by stating that BCG at birth should be maintained in at least all leprosy high-burden regions. Literature shows that several vaccination interventions with other immunoprophylactic agents demonstrate similar or slightly less efficacy in leprosy risk reduction compared with BCG. However, most of these studies do not exclusively focus on post-exposure prophylaxis. Two vaccines are considered future candidates for leprosy prophylaxis: Mycobacterium indicus pranii (MiP) and LepVax. For chemoprophylaxis, trials were performed with dapsone/acedapsone, rifampicin, and ROM, a combination of rifampicin, ofloxacin, and minocycline. Single-dose rifampicin is favored as post-exposure prophylaxis, abbreviated as SDR-PEP. It demonstrated a protective effect of 57% in the first two years after administration to contacts of leprosy patients. It is inexpensive, and adverse events are rare. The risk of SDR-PEP inducing rifampicin resistance is considered negligible, but continuous monitoring in accordance with WHO policies should be encouraged. The integration of contact screening and SDR-PEP administration into different leprosy control programs was found to be feasible and well accepted. Since 2018, SDR-PEP is included in the WHO Guidelines for the Diagnosis, Treatment and Prevention of Leprosy.
Conclusion: Progress has been made in the areas of chemoprophylaxis and immunoprophylaxis to prevent leprosy in contacts of patients. Investing in vaccine studies, like LepVax and MiP, and increasing harmonization between tuberculosis (TB) and leprosy research groups is important. SDR-PEP is promising as a chemoprophylactic agent, and further implementation should be promoted. More chemoprophylaxis research is needed on: enhanced medication regimens; interventions in varying (epidemiological) settings, including focal mass drug administration (fMDA); specific approaches per contact type; combinations with screening variations and field-friendly rapid tests, if available in the future; community and health staff education; ongoing antibiotic resistance surveillance; and administering chemoprophylaxis with SDR-PEP prior to BCG administration. Additionally, both leprosy prophylactic drug registration nationally and prophylactic drug availability globally at low or no cost are important for the implementation and further upscaling of preventive measures against leprosy, such as SDR-PEP and new vaccines.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
