Tracey Goldstein, Manjunatha N Belaganahalli, Eddy K Syaluha, Jean-Paul K Lukusa, Denise J Greig, Simon J Anthony, Alexandre Tremeau-Bravard, Riddhi Thakkar, Adrian Caciula, Nischay Mishra, W Ian Lipkin, Jasjeet K Dhanota, Brett R Smith, Victoria M Ontiveros, Nistara Randhawa, Michael Cranfield, Christine K Johnson, Kirsten V Gilardi, Jonna A K Mazet
{"title":"在2018年埃博拉病毒病爆发之前,埃博拉病毒在刚果民主共和国东部扩散到人群中。","authors":"Tracey Goldstein, Manjunatha N Belaganahalli, Eddy K Syaluha, Jean-Paul K Lukusa, Denise J Greig, Simon J Anthony, Alexandre Tremeau-Bravard, Riddhi Thakkar, Adrian Caciula, Nischay Mishra, W Ian Lipkin, Jasjeet K Dhanota, Brett R Smith, Victoria M Ontiveros, Nistara Randhawa, Michael Cranfield, Christine K Johnson, Kirsten V Gilardi, Jonna A K Mazet","doi":"10.1186/s42522-020-00028-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The second largest Ebola virus disease (EVD) outbreak began in the Democratic Republic of Congo in July 2018 in North Kivu Province. Data suggest the outbreak is not epidemiologically linked to the 2018 outbreak in Equateur Province, and that independent introduction of Ebola virus (EBOV) into humans occurred. We tested for antibodies to ebolaviruses in febrile patients seeking care in North Kivu Province prior to the EVD outbreak.</p><p><strong>Methods: </strong>Patients were enrolled between May 2017 and April 2018, before the declared start of the outbreak in eastern DRC. Questionnaires were administered to collect demographic and behavioural information to identify risk factors for exposure. Biological samples were evaluated for ebolavirus nucleic acid, and for antibodies to ebolaviruses. Prevalence of exposure was calculated, and demographic factors evaluated for associations with ebolavirus serostatus.</p><p><strong>Results: </strong>Samples were collected and tested from 272 people seeking care in the Rutshuru Health Zone in North Kivu Province. All patients were negative for filoviruses by PCR. Intial screening by indirect ELISA found that 30 people were reactive to EBOV-rGP. Results were supported by detection of ebolavirus reactive linear peptides using the Serochip platform. Differential screening of all reactive serum samples against the rGP of all six ebolaviruses and Marburg virus (MARV) showed that 29 people exhibited the strongest reactivity to EBOV and one to Bombali virus (BOMV), and western blotting confirmed results. Titers ranged from 1:100 to 1:12,800. Although both sexes and all ages tested positive for antibodies, women were significantly more likely to be positive and the majority of positives were in February 2018.</p><p><strong>Conclusions: </strong>We provide the first documented evidence of exposure to Ebola virus in people in eastern DRC. We detected antibodies to EBOV in 10% of febrile patients seeking healthcare prior to the declaration of the 2018-2020 outbreak, suggesting early cases may have been missed or exposure ocurred without associated illness. We also report the first known detection of antibodies to BOMV, previously detected in bats in West and East Africa, and show that human exposure to BOMV has occurred. Our data suggest human exposure to ebolaviruses may be more frequent and geographically widespread.</p>","PeriodicalId":19490,"journal":{"name":"One Health Outlook","volume":"2 1","pages":"21"},"PeriodicalIF":0.0000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s42522-020-00028-1","citationCount":"5","resultStr":"{\"title\":\"Spillover of ebolaviruses into people in eastern Democratic Republic of Congo prior to the 2018 Ebola virus disease outbreak.\",\"authors\":\"Tracey Goldstein, Manjunatha N Belaganahalli, Eddy K Syaluha, Jean-Paul K Lukusa, Denise J Greig, Simon J Anthony, Alexandre Tremeau-Bravard, Riddhi Thakkar, Adrian Caciula, Nischay Mishra, W Ian Lipkin, Jasjeet K Dhanota, Brett R Smith, Victoria M Ontiveros, Nistara Randhawa, Michael Cranfield, Christine K Johnson, Kirsten V Gilardi, Jonna A K Mazet\",\"doi\":\"10.1186/s42522-020-00028-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The second largest Ebola virus disease (EVD) outbreak began in the Democratic Republic of Congo in July 2018 in North Kivu Province. Data suggest the outbreak is not epidemiologically linked to the 2018 outbreak in Equateur Province, and that independent introduction of Ebola virus (EBOV) into humans occurred. We tested for antibodies to ebolaviruses in febrile patients seeking care in North Kivu Province prior to the EVD outbreak.</p><p><strong>Methods: </strong>Patients were enrolled between May 2017 and April 2018, before the declared start of the outbreak in eastern DRC. Questionnaires were administered to collect demographic and behavioural information to identify risk factors for exposure. Biological samples were evaluated for ebolavirus nucleic acid, and for antibodies to ebolaviruses. Prevalence of exposure was calculated, and demographic factors evaluated for associations with ebolavirus serostatus.</p><p><strong>Results: </strong>Samples were collected and tested from 272 people seeking care in the Rutshuru Health Zone in North Kivu Province. All patients were negative for filoviruses by PCR. Intial screening by indirect ELISA found that 30 people were reactive to EBOV-rGP. Results were supported by detection of ebolavirus reactive linear peptides using the Serochip platform. Differential screening of all reactive serum samples against the rGP of all six ebolaviruses and Marburg virus (MARV) showed that 29 people exhibited the strongest reactivity to EBOV and one to Bombali virus (BOMV), and western blotting confirmed results. Titers ranged from 1:100 to 1:12,800. Although both sexes and all ages tested positive for antibodies, women were significantly more likely to be positive and the majority of positives were in February 2018.</p><p><strong>Conclusions: </strong>We provide the first documented evidence of exposure to Ebola virus in people in eastern DRC. We detected antibodies to EBOV in 10% of febrile patients seeking healthcare prior to the declaration of the 2018-2020 outbreak, suggesting early cases may have been missed or exposure ocurred without associated illness. We also report the first known detection of antibodies to BOMV, previously detected in bats in West and East Africa, and show that human exposure to BOMV has occurred. Our data suggest human exposure to ebolaviruses may be more frequent and geographically widespread.</p>\",\"PeriodicalId\":19490,\"journal\":{\"name\":\"One Health Outlook\",\"volume\":\"2 1\",\"pages\":\"21\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1186/s42522-020-00028-1\",\"citationCount\":\"5\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"One Health Outlook\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s42522-020-00028-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/11/4 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"One Health Outlook","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42522-020-00028-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/11/4 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Spillover of ebolaviruses into people in eastern Democratic Republic of Congo prior to the 2018 Ebola virus disease outbreak.
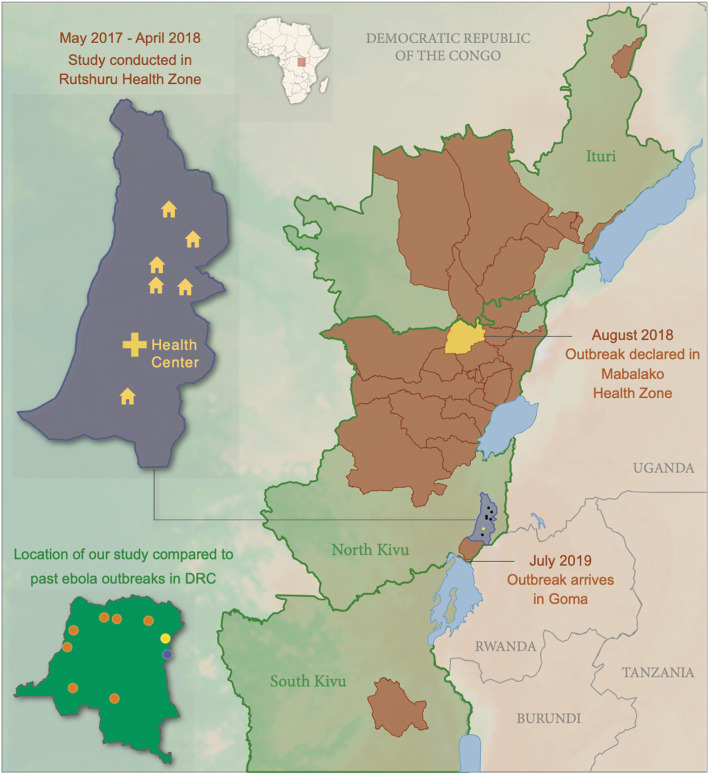
Background: The second largest Ebola virus disease (EVD) outbreak began in the Democratic Republic of Congo in July 2018 in North Kivu Province. Data suggest the outbreak is not epidemiologically linked to the 2018 outbreak in Equateur Province, and that independent introduction of Ebola virus (EBOV) into humans occurred. We tested for antibodies to ebolaviruses in febrile patients seeking care in North Kivu Province prior to the EVD outbreak.
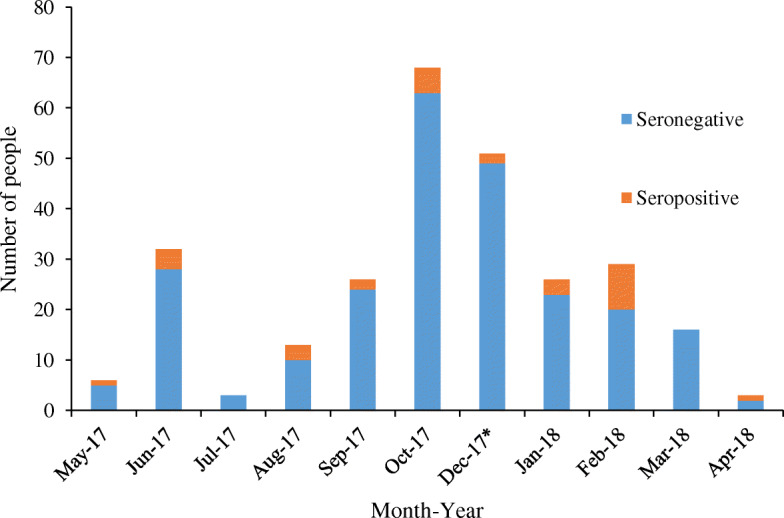
Methods: Patients were enrolled between May 2017 and April 2018, before the declared start of the outbreak in eastern DRC. Questionnaires were administered to collect demographic and behavioural information to identify risk factors for exposure. Biological samples were evaluated for ebolavirus nucleic acid, and for antibodies to ebolaviruses. Prevalence of exposure was calculated, and demographic factors evaluated for associations with ebolavirus serostatus.
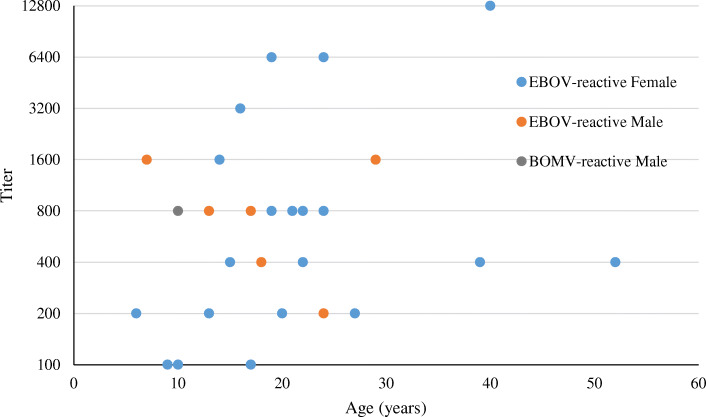
Results: Samples were collected and tested from 272 people seeking care in the Rutshuru Health Zone in North Kivu Province. All patients were negative for filoviruses by PCR. Intial screening by indirect ELISA found that 30 people were reactive to EBOV-rGP. Results were supported by detection of ebolavirus reactive linear peptides using the Serochip platform. Differential screening of all reactive serum samples against the rGP of all six ebolaviruses and Marburg virus (MARV) showed that 29 people exhibited the strongest reactivity to EBOV and one to Bombali virus (BOMV), and western blotting confirmed results. Titers ranged from 1:100 to 1:12,800. Although both sexes and all ages tested positive for antibodies, women were significantly more likely to be positive and the majority of positives were in February 2018.
Conclusions: We provide the first documented evidence of exposure to Ebola virus in people in eastern DRC. We detected antibodies to EBOV in 10% of febrile patients seeking healthcare prior to the declaration of the 2018-2020 outbreak, suggesting early cases may have been missed or exposure ocurred without associated illness. We also report the first known detection of antibodies to BOMV, previously detected in bats in West and East Africa, and show that human exposure to BOMV has occurred. Our data suggest human exposure to ebolaviruses may be more frequent and geographically widespread.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
