Mohamed M Soliman, Debkumar Sarkar, Ilya Glezerman, Majid Maybody
{"title":"肝动脉栓塞后术中非造影剂计算机断层成像的发现与造影剂肾病的发展有关。","authors":"Mohamed M Soliman, Debkumar Sarkar, Ilya Glezerman, Majid Maybody","doi":"10.5527/wjn.v9.i2.33","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Contrast-induced nephropathy (CIN) is a reversible form of acute kidney injury that occurs within 48-72 h of exposure to intravascular contrast material. CIN is the third leading cause of hospital-acquired acute kidney injury and accounts for 12% of such cases. Risk factors for CIN development can be divided into patient- and procedure-related. The former includes pre-existing chronic renal insufficiency and diabetes mellitus. The latter includes high contrast volume and repeated exposure over 72 h. The incidence of CIN is relatively low (up to 5%) in patients with intact renal function. However, in patients with known chronic renal insufficiency, the incidence can reach up to 27%.</p><p><strong>Aim: </strong>To examine the association between renal enhancement pattern on non-contrast enhanced computed tomographic (CT) images obtained immediately following hepatic artery embolization with development of CIN.</p><p><strong>Methods: </strong>Retrospective review of all patients who underwent hepatic artery embolization between 01/2010 and 01/2011 (<i>n</i> = 162) was performed. Patients without intraprocedural CT imaging (<i>n</i> = 51), combined embolization/ablation (<i>n</i> = 6) and those with chronic kidney disease (<i>n</i> = 21) were excluded. The study group comprised of 84 patients with 106 procedures. CIN was defined as 25% increase above baseline serum creatinine or absolute increase ≥ 0.5 mg/dL within 72 h post-embolization. Post-embolization CT was reviewed for renal enhancement patterns and presence of renal artery calcifications. The association between non-contrast CT findings and CIN development was examined by Fisher's Exact Test.</p><p><strong>Results: </strong>CIN occurred in 11/106 (10.3%) procedures (Group A, <i>n</i> = 10). The renal enhancement pattern in patients who did not experience CIN (Group B, <i>n</i> = 74 with 95/106 procedures) was late excretory in 93/95 (98%) and early excretory (EE) in 2/95 (2%). However, in Group A, there was a significantly higher rate of EE pattern (6/11, 55%) compared to late excretory pattern (5/11) (<i>P</i> < 0.001). A significantly higher percentage of patients that developed CIN had renal artery calcifications (6/11 <i>vs</i> 20/95, 55% <i>vs</i> 21%, <i>P</i> = 0.02).</p><p><strong>Conclusion: </strong>A hyperdense renal parenchyma relative to surrounding skeletal muscle (EE pattern) and presence of renal artery calcifications on immediate post-HAE non-contrast CT images in patients with low risk for CIN are independently associated with CIN development.</p>","PeriodicalId":23745,"journal":{"name":"World Journal of Nephrology","volume":"9 2","pages":"33-42"},"PeriodicalIF":0.0000,"publicationDate":"2020-11-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a0/22/WJN-9-33.PMC7701934.pdf","citationCount":"0","resultStr":"{\"title\":\"Findings on intraprocedural non-contrast computed tomographic imaging following hepatic artery embolization are associated with development of contrast-induced nephropathy.\",\"authors\":\"Mohamed M Soliman, Debkumar Sarkar, Ilya Glezerman, Majid Maybody\",\"doi\":\"10.5527/wjn.v9.i2.33\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Contrast-induced nephropathy (CIN) is a reversible form of acute kidney injury that occurs within 48-72 h of exposure to intravascular contrast material. CIN is the third leading cause of hospital-acquired acute kidney injury and accounts for 12% of such cases. Risk factors for CIN development can be divided into patient- and procedure-related. The former includes pre-existing chronic renal insufficiency and diabetes mellitus. The latter includes high contrast volume and repeated exposure over 72 h. The incidence of CIN is relatively low (up to 5%) in patients with intact renal function. However, in patients with known chronic renal insufficiency, the incidence can reach up to 27%.</p><p><strong>Aim: </strong>To examine the association between renal enhancement pattern on non-contrast enhanced computed tomographic (CT) images obtained immediately following hepatic artery embolization with development of CIN.</p><p><strong>Methods: </strong>Retrospective review of all patients who underwent hepatic artery embolization between 01/2010 and 01/2011 (<i>n</i> = 162) was performed. Patients without intraprocedural CT imaging (<i>n</i> = 51), combined embolization/ablation (<i>n</i> = 6) and those with chronic kidney disease (<i>n</i> = 21) were excluded. The study group comprised of 84 patients with 106 procedures. CIN was defined as 25% increase above baseline serum creatinine or absolute increase ≥ 0.5 mg/dL within 72 h post-embolization. Post-embolization CT was reviewed for renal enhancement patterns and presence of renal artery calcifications. The association between non-contrast CT findings and CIN development was examined by Fisher's Exact Test.</p><p><strong>Results: </strong>CIN occurred in 11/106 (10.3%) procedures (Group A, <i>n</i> = 10). The renal enhancement pattern in patients who did not experience CIN (Group B, <i>n</i> = 74 with 95/106 procedures) was late excretory in 93/95 (98%) and early excretory (EE) in 2/95 (2%). However, in Group A, there was a significantly higher rate of EE pattern (6/11, 55%) compared to late excretory pattern (5/11) (<i>P</i> < 0.001). A significantly higher percentage of patients that developed CIN had renal artery calcifications (6/11 <i>vs</i> 20/95, 55% <i>vs</i> 21%, <i>P</i> = 0.02).</p><p><strong>Conclusion: </strong>A hyperdense renal parenchyma relative to surrounding skeletal muscle (EE pattern) and presence of renal artery calcifications on immediate post-HAE non-contrast CT images in patients with low risk for CIN are independently associated with CIN development.</p>\",\"PeriodicalId\":23745,\"journal\":{\"name\":\"World Journal of Nephrology\",\"volume\":\"9 2\",\"pages\":\"33-42\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-11-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a0/22/WJN-9-33.PMC7701934.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Nephrology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5527/wjn.v9.i2.33\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5527/wjn.v9.i2.33","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:造影剂肾病(CIN)是一种可逆的急性肾损伤,发生在血管内造影剂暴露48-72小时内。CIN是医院获得性急性肾损伤的第三大原因,占此类病例的12%。CIN发展的危险因素可分为与患者相关和与手术相关。前者包括先前存在的慢性肾功能不全和糖尿病。后者包括高造影剂体积和超过72小时的反复暴露。在肾功能完好的患者中,CIN的发生率相对较低(高达5%)。然而,在已知的慢性肾功能不全患者中,发病率可高达27%。目的:探讨肝动脉栓塞后立即获得的非增强计算机断层扫描(CT)肾脏增强模式与CIN发展的关系。方法:回顾性分析2010年1月至2011年1月间接受肝动脉栓塞治疗的162例患者。排除无术中CT影像的患者(51例)、联合栓塞/消融(6例)和慢性肾脏疾病患者(21例)。研究组包括84例患者,106例手术。CIN定义为栓塞后72小时内血清肌酐比基线升高25%或绝对升高≥0.5 mg/dL。栓塞后的CT检查肾强化模式和肾动脉钙化的存在。通过Fisher精确检验检查非对比CT表现与CIN发展之间的关系。结果:11/106(10.3%)例手术发生CIN (A组,n = 10)。未经历CIN的患者(B组,n = 74, 95/106次手术)的肾脏增强模式为93/95(98%)晚期排泄,2/95(2%)早期排泄。然而,在A组,EE模式的发生率(6/ 11,55%)显著高于晚期排泄模式(5/11)(P < 0.001)。发生CIN的患者发生肾动脉钙化的比例明显更高(6/11 vs 20/95, 55% vs 21%, P = 0.02)。结论:相对于周围骨骼肌的高密度肾实质(EE型)和肾动脉钙化在低风险CIN患者hae后立即非对比CT图像上的存在与CIN的发展独立相关。
Findings on intraprocedural non-contrast computed tomographic imaging following hepatic artery embolization are associated with development of contrast-induced nephropathy.
Background: Contrast-induced nephropathy (CIN) is a reversible form of acute kidney injury that occurs within 48-72 h of exposure to intravascular contrast material. CIN is the third leading cause of hospital-acquired acute kidney injury and accounts for 12% of such cases. Risk factors for CIN development can be divided into patient- and procedure-related. The former includes pre-existing chronic renal insufficiency and diabetes mellitus. The latter includes high contrast volume and repeated exposure over 72 h. The incidence of CIN is relatively low (up to 5%) in patients with intact renal function. However, in patients with known chronic renal insufficiency, the incidence can reach up to 27%.
Aim: To examine the association between renal enhancement pattern on non-contrast enhanced computed tomographic (CT) images obtained immediately following hepatic artery embolization with development of CIN.
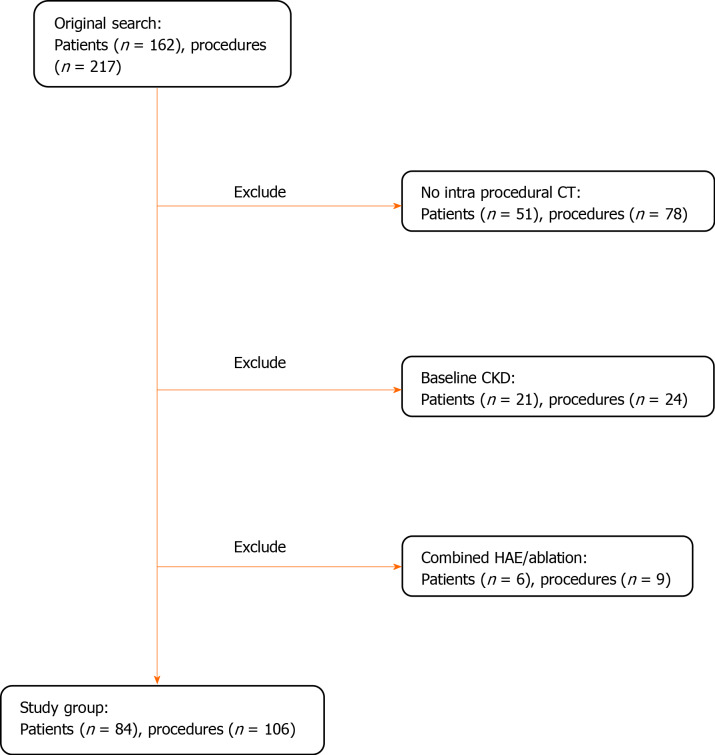
Methods: Retrospective review of all patients who underwent hepatic artery embolization between 01/2010 and 01/2011 (n = 162) was performed. Patients without intraprocedural CT imaging (n = 51), combined embolization/ablation (n = 6) and those with chronic kidney disease (n = 21) were excluded. The study group comprised of 84 patients with 106 procedures. CIN was defined as 25% increase above baseline serum creatinine or absolute increase ≥ 0.5 mg/dL within 72 h post-embolization. Post-embolization CT was reviewed for renal enhancement patterns and presence of renal artery calcifications. The association between non-contrast CT findings and CIN development was examined by Fisher's Exact Test.
Results: CIN occurred in 11/106 (10.3%) procedures (Group A, n = 10). The renal enhancement pattern in patients who did not experience CIN (Group B, n = 74 with 95/106 procedures) was late excretory in 93/95 (98%) and early excretory (EE) in 2/95 (2%). However, in Group A, there was a significantly higher rate of EE pattern (6/11, 55%) compared to late excretory pattern (5/11) (P < 0.001). A significantly higher percentage of patients that developed CIN had renal artery calcifications (6/11 vs 20/95, 55% vs 21%, P = 0.02).
Conclusion: A hyperdense renal parenchyma relative to surrounding skeletal muscle (EE pattern) and presence of renal artery calcifications on immediate post-HAE non-contrast CT images in patients with low risk for CIN are independently associated with CIN development.





 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
