Robyn Schickler , Diana Crabtree-Sokol , Jasmine Patel , Nicole Bender , Anita L. Nelson , Brian T. Nguyen
{"title":"肌内储存醋酸甲孕酮作为一种自我桥接紧急避孕药的潜力","authors":"Robyn Schickler , Diana Crabtree-Sokol , Jasmine Patel , Nicole Bender , Anita L. Nelson , Brian T. Nguyen","doi":"10.1016/j.conx.2020.100050","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>To examine the rate of ovulatory disruption when intramuscular depot medroxyprogesterone acetate (DMPA) is administered across graded stages of dominant follicle development.</p></div><div><h3>Study design</h3><p>We assigned enrolled participants to one of three preassigned dominant follicle size groups: 12-14 mm, 15–17 mm and ≥<!--> <!-->18 mm. We followed dominant follicles via serial transvaginal ultrasound (TVUS) until the follicles reached their assigned size, at which time we administered DMPA. For 5 consecutive days thereafter, we followed the follicles via TVUS to observe follicle rupture and obtained serum luteinizing hormone (LH), estradiol, and progesterone concentrations. In the following 2 weeks, we collected serum progesterone concentrations twice weekly to detect possible ovulatory delay or dysfunction. We also collected serum medroxyprogesterone acetate (MPA) concentrations at 1 and 24 h after DMPA administration to examine against ovulatory outcomes.</p></div><div><h3>Results</h3><p>Twenty-six of 29 enrolled women completed the study. DMPA suppressed ovulation in 17/26 (65%) and caused ovulatory dysfunction in 1/26 (4%) participants. Larger follicles were more likely to rupture despite DMPA (12–14 mm: 0/10 (0%); 15–17 mm: 3/10 (30%); ≥<!--> <!-->18 mm: 6/6 (100%); p < .01). Pre-DMPA LH concentrations ranged from 13.8 to 93.7 IU/L (mean 49.0 IU/L) in cases of follicle rupture. We observed no cases of follicle rupture when DMPA was administered through cycle day 12. All 24-h MPA concentrations exceeded those needed for ovulation suppression.</p></div><div><h3>Conclusion</h3><p>DMPA suppressed and additionally disrupted ovulation in 65% and 4% of observed cycles, respectively. DMPA may provide effective emergency contraception as well as ongoing contraception if administered prior to an expected ovulation and specifically before the LH surge.</p></div><div><h3>Implications</h3><p>DMPA may be an alternative form of emergency contraception that can also self-bridge to ongoing contraception. As ovulation was not observed among any follicles when DMPA was given through cycle day 12, women who initiate DMPA up through cycle day 12 may not require backup contraception.</p></div>","PeriodicalId":10655,"journal":{"name":"Contraception: X","volume":"3 ","pages":"Article 100050"},"PeriodicalIF":0.0000,"publicationDate":"2021-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.conx.2020.100050","citationCount":"1","resultStr":"{\"title\":\"The potential for intramuscular depot medroxyprogesterone acetate as a self-bridging emergency contraceptive\",\"authors\":\"Robyn Schickler , Diana Crabtree-Sokol , Jasmine Patel , Nicole Bender , Anita L. Nelson , Brian T. Nguyen\",\"doi\":\"10.1016/j.conx.2020.100050\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Objective</h3><p>To examine the rate of ovulatory disruption when intramuscular depot medroxyprogesterone acetate (DMPA) is administered across graded stages of dominant follicle development.</p></div><div><h3>Study design</h3><p>We assigned enrolled participants to one of three preassigned dominant follicle size groups: 12-14 mm, 15–17 mm and ≥<!--> <!-->18 mm. We followed dominant follicles via serial transvaginal ultrasound (TVUS) until the follicles reached their assigned size, at which time we administered DMPA. For 5 consecutive days thereafter, we followed the follicles via TVUS to observe follicle rupture and obtained serum luteinizing hormone (LH), estradiol, and progesterone concentrations. In the following 2 weeks, we collected serum progesterone concentrations twice weekly to detect possible ovulatory delay or dysfunction. We also collected serum medroxyprogesterone acetate (MPA) concentrations at 1 and 24 h after DMPA administration to examine against ovulatory outcomes.</p></div><div><h3>Results</h3><p>Twenty-six of 29 enrolled women completed the study. DMPA suppressed ovulation in 17/26 (65%) and caused ovulatory dysfunction in 1/26 (4%) participants. Larger follicles were more likely to rupture despite DMPA (12–14 mm: 0/10 (0%); 15–17 mm: 3/10 (30%); ≥<!--> <!-->18 mm: 6/6 (100%); p < .01). Pre-DMPA LH concentrations ranged from 13.8 to 93.7 IU/L (mean 49.0 IU/L) in cases of follicle rupture. We observed no cases of follicle rupture when DMPA was administered through cycle day 12. All 24-h MPA concentrations exceeded those needed for ovulation suppression.</p></div><div><h3>Conclusion</h3><p>DMPA suppressed and additionally disrupted ovulation in 65% and 4% of observed cycles, respectively. DMPA may provide effective emergency contraception as well as ongoing contraception if administered prior to an expected ovulation and specifically before the LH surge.</p></div><div><h3>Implications</h3><p>DMPA may be an alternative form of emergency contraception that can also self-bridge to ongoing contraception. As ovulation was not observed among any follicles when DMPA was given through cycle day 12, women who initiate DMPA up through cycle day 12 may not require backup contraception.</p></div>\",\"PeriodicalId\":10655,\"journal\":{\"name\":\"Contraception: X\",\"volume\":\"3 \",\"pages\":\"Article 100050\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1016/j.conx.2020.100050\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Contraception: X\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2590151620300332\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/12/3 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Contraception: X","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590151620300332","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/12/3 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
The potential for intramuscular depot medroxyprogesterone acetate as a self-bridging emergency contraceptive
Objective
To examine the rate of ovulatory disruption when intramuscular depot medroxyprogesterone acetate (DMPA) is administered across graded stages of dominant follicle development.
Study design
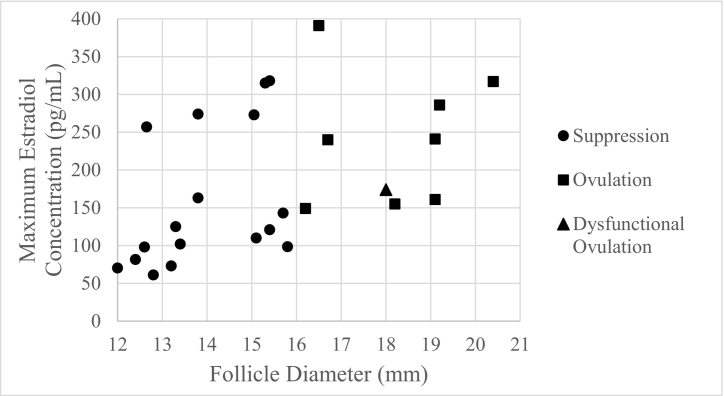
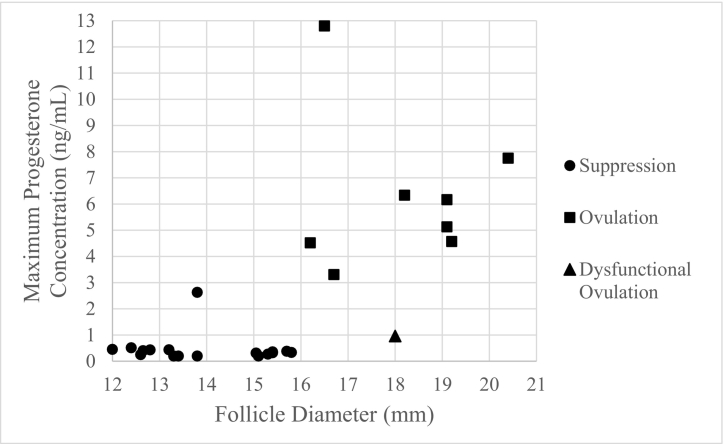
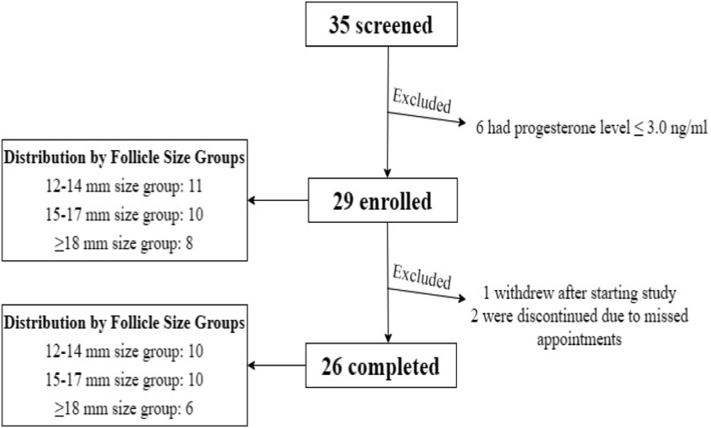
We assigned enrolled participants to one of three preassigned dominant follicle size groups: 12-14 mm, 15–17 mm and ≥ 18 mm. We followed dominant follicles via serial transvaginal ultrasound (TVUS) until the follicles reached their assigned size, at which time we administered DMPA. For 5 consecutive days thereafter, we followed the follicles via TVUS to observe follicle rupture and obtained serum luteinizing hormone (LH), estradiol, and progesterone concentrations. In the following 2 weeks, we collected serum progesterone concentrations twice weekly to detect possible ovulatory delay or dysfunction. We also collected serum medroxyprogesterone acetate (MPA) concentrations at 1 and 24 h after DMPA administration to examine against ovulatory outcomes.
Results
Twenty-six of 29 enrolled women completed the study. DMPA suppressed ovulation in 17/26 (65%) and caused ovulatory dysfunction in 1/26 (4%) participants. Larger follicles were more likely to rupture despite DMPA (12–14 mm: 0/10 (0%); 15–17 mm: 3/10 (30%); ≥ 18 mm: 6/6 (100%); p < .01). Pre-DMPA LH concentrations ranged from 13.8 to 93.7 IU/L (mean 49.0 IU/L) in cases of follicle rupture. We observed no cases of follicle rupture when DMPA was administered through cycle day 12. All 24-h MPA concentrations exceeded those needed for ovulation suppression.
Conclusion
DMPA suppressed and additionally disrupted ovulation in 65% and 4% of observed cycles, respectively. DMPA may provide effective emergency contraception as well as ongoing contraception if administered prior to an expected ovulation and specifically before the LH surge.
Implications
DMPA may be an alternative form of emergency contraception that can also self-bridge to ongoing contraception. As ovulation was not observed among any follicles when DMPA was given through cycle day 12, women who initiate DMPA up through cycle day 12 may not require backup contraception.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
