Arash Mollaeian, Nina Chan, Rohit Aloor, Jeffery S Iding, Lois J Arend, Seyed Hootan Forghani Saeidabadi, Christopher J Haas
{"title":"显微镜下anca阴性多血管炎伴弥漫性肺泡出血,伪装成充血性心力衰竭。","authors":"Arash Mollaeian, Nina Chan, Rohit Aloor, Jeffery S Iding, Lois J Arend, Seyed Hootan Forghani Saeidabadi, Christopher J Haas","doi":"10.1186/s13317-020-00143-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Microscopic polyangiitis (MPA) is a subtype of anti-neutrophil cytoplasmic antibody-associated vasculitis (AAV), involving small and medium sized vessels, often affecting the kidneys and lungs. Anti-neutrophil cytoplasmic antibody (ANCA) is detected in up to 90% of cases of MPA and its detection helps guide diagnosis, however cases of ANCA-negative MPA have been reported, hence definitive diagnosis relies on tissue biopsy.</p><p><strong>Case report: </strong>A 23-year-old man was evaluated for dyspnea and pleuritic chest pain, and found to have bilateral intra-alveolar opacities and hilar adenopathy. Diagnostic work up revealed positive anti-nuclear antibodies (ANA) and negative ANCA, which in the setting of a non-classical presentation, delayed diagnosis and appropriate treatment. Due to persistent symptoms and a high suspicion for autoimmune disease with pulmonary-renal syndrome, he underwent lung biopsy which revealed intra-alveolar hemorrhage and capillaritis indicative of microscopic polyangiitis (MPA). Surprisingly, kidney biopsy was not typical of classic MPA, but revealed less common features. Due to therapeutic noncompliance he was readmitted multiple times thereafter with rare complications of MPA such as acute pancreatitis and hemorrhagic pericardial effusion with tamponade.</p><p><strong>Conclusion: </strong>This case serves as an important clinical reminder to consider AAV even in those with negative ANCA serologies and a high suspicion for pulmonary-renal syndrome. It also demonstrates the high morbidity in cases of diagnostic delay and inadequate treatment.</p>","PeriodicalId":8655,"journal":{"name":"Auto-Immunity Highlights","volume":"12 1","pages":"1"},"PeriodicalIF":0.0000,"publicationDate":"2021-01-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7788985/pdf/","citationCount":"3","resultStr":"{\"title\":\"ANCA-negative microscopic polyangiitis with diffuse alveolar hemorrhage masquerading as congestive heart failure.\",\"authors\":\"Arash Mollaeian, Nina Chan, Rohit Aloor, Jeffery S Iding, Lois J Arend, Seyed Hootan Forghani Saeidabadi, Christopher J Haas\",\"doi\":\"10.1186/s13317-020-00143-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Microscopic polyangiitis (MPA) is a subtype of anti-neutrophil cytoplasmic antibody-associated vasculitis (AAV), involving small and medium sized vessels, often affecting the kidneys and lungs. Anti-neutrophil cytoplasmic antibody (ANCA) is detected in up to 90% of cases of MPA and its detection helps guide diagnosis, however cases of ANCA-negative MPA have been reported, hence definitive diagnosis relies on tissue biopsy.</p><p><strong>Case report: </strong>A 23-year-old man was evaluated for dyspnea and pleuritic chest pain, and found to have bilateral intra-alveolar opacities and hilar adenopathy. Diagnostic work up revealed positive anti-nuclear antibodies (ANA) and negative ANCA, which in the setting of a non-classical presentation, delayed diagnosis and appropriate treatment. Due to persistent symptoms and a high suspicion for autoimmune disease with pulmonary-renal syndrome, he underwent lung biopsy which revealed intra-alveolar hemorrhage and capillaritis indicative of microscopic polyangiitis (MPA). Surprisingly, kidney biopsy was not typical of classic MPA, but revealed less common features. Due to therapeutic noncompliance he was readmitted multiple times thereafter with rare complications of MPA such as acute pancreatitis and hemorrhagic pericardial effusion with tamponade.</p><p><strong>Conclusion: </strong>This case serves as an important clinical reminder to consider AAV even in those with negative ANCA serologies and a high suspicion for pulmonary-renal syndrome. It also demonstrates the high morbidity in cases of diagnostic delay and inadequate treatment.</p>\",\"PeriodicalId\":8655,\"journal\":{\"name\":\"Auto-Immunity Highlights\",\"volume\":\"12 1\",\"pages\":\"1\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-01-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7788985/pdf/\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Auto-Immunity Highlights\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13317-020-00143-z\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Auto-Immunity Highlights","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13317-020-00143-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
ANCA-negative microscopic polyangiitis with diffuse alveolar hemorrhage masquerading as congestive heart failure.
Background: Microscopic polyangiitis (MPA) is a subtype of anti-neutrophil cytoplasmic antibody-associated vasculitis (AAV), involving small and medium sized vessels, often affecting the kidneys and lungs. Anti-neutrophil cytoplasmic antibody (ANCA) is detected in up to 90% of cases of MPA and its detection helps guide diagnosis, however cases of ANCA-negative MPA have been reported, hence definitive diagnosis relies on tissue biopsy.
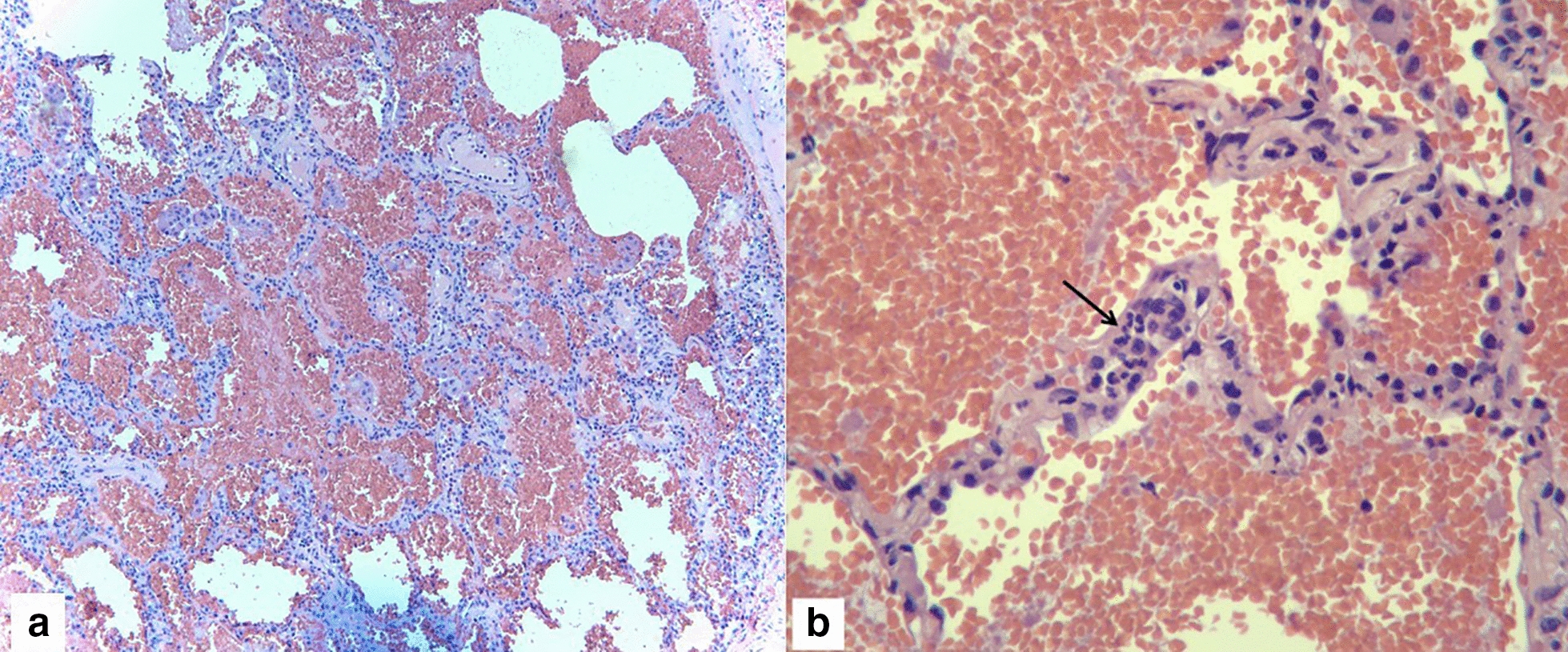
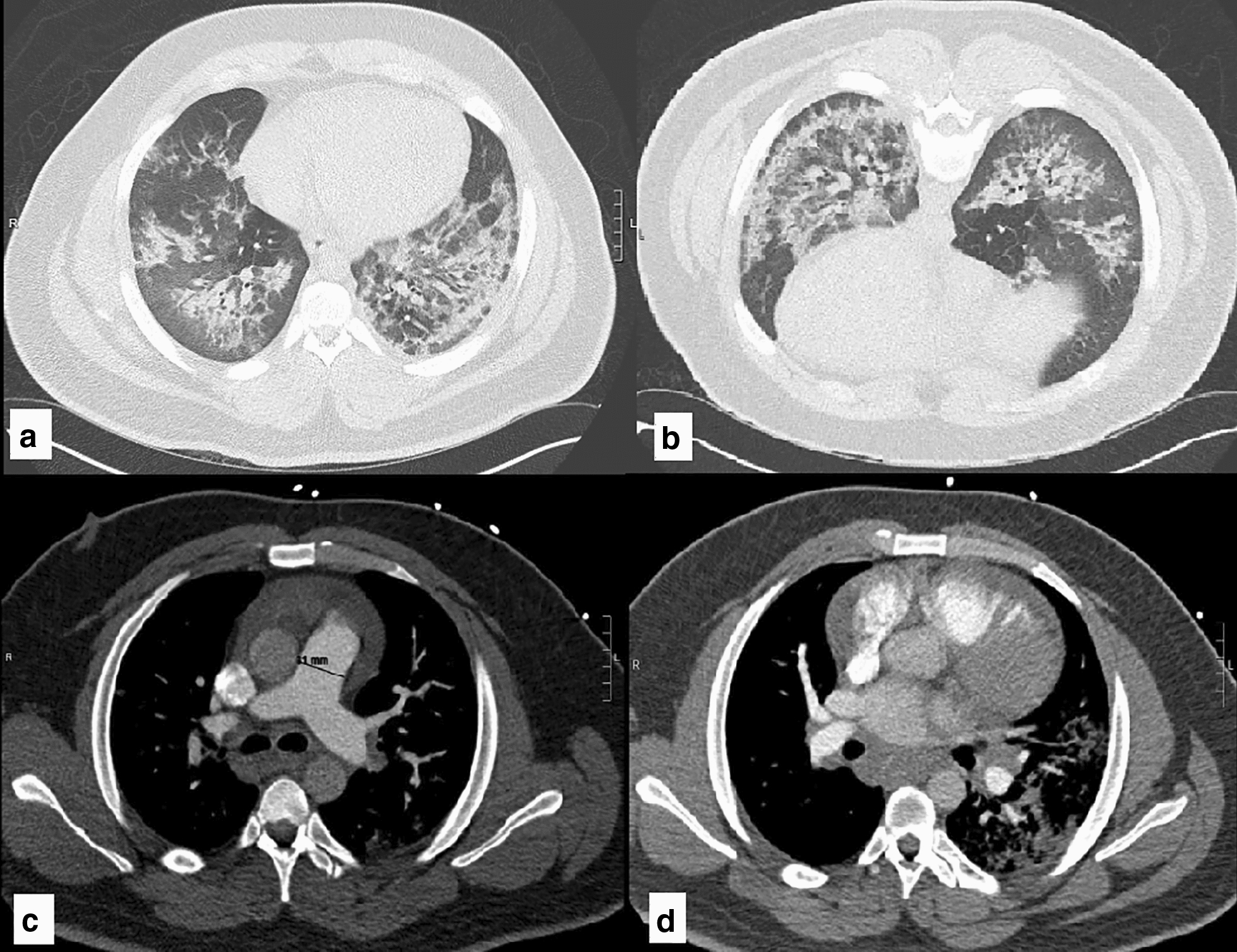
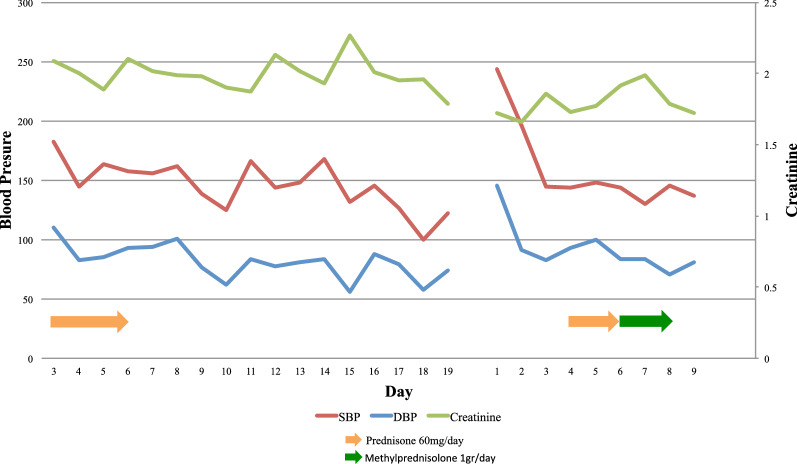
Case report: A 23-year-old man was evaluated for dyspnea and pleuritic chest pain, and found to have bilateral intra-alveolar opacities and hilar adenopathy. Diagnostic work up revealed positive anti-nuclear antibodies (ANA) and negative ANCA, which in the setting of a non-classical presentation, delayed diagnosis and appropriate treatment. Due to persistent symptoms and a high suspicion for autoimmune disease with pulmonary-renal syndrome, he underwent lung biopsy which revealed intra-alveolar hemorrhage and capillaritis indicative of microscopic polyangiitis (MPA). Surprisingly, kidney biopsy was not typical of classic MPA, but revealed less common features. Due to therapeutic noncompliance he was readmitted multiple times thereafter with rare complications of MPA such as acute pancreatitis and hemorrhagic pericardial effusion with tamponade.
Conclusion: This case serves as an important clinical reminder to consider AAV even in those with negative ANCA serologies and a high suspicion for pulmonary-renal syndrome. It also demonstrates the high morbidity in cases of diagnostic delay and inadequate treatment.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
