Melhem M Solh, Gabriel Hinojosa, Justin Laporte, Scott R Solomon, Lawrence E Morris, Xu Zhang, H Kent Holland, Asad Bashey
{"title":"基于Melphalan的低强度调节用于移植t - hla -单倍体外周血干细胞与移植后环磷酰胺治疗血液恶性肿瘤患者的II期试验","authors":"Melhem M Solh, Gabriel Hinojosa, Justin Laporte, Scott R Solomon, Lawrence E Morris, Xu Zhang, H Kent Holland, Asad Bashey","doi":"10.1155/2021/8868142","DOIUrl":null,"url":null,"abstract":"<p><p>T-replete haploidentical donor transplants using posttransplant cyclophosphamide (haplo) have greatly expanded donor availability and are increasingly utilized. Haplo were originally performed using truly nonmyeloablative conditioning and a bone marrow graft. We have also developed myeloablative conditioning and peripheral blood stem cell (PBSC) grafts for use with haplo. However, some patients may not tolerate myeloablative conditioning but may still benefit from a more dose-intensified preparative regimen to control malignancy and diminish graft rejection. To this end, we enrolled 25 patients on a prospective phase II trial utilizing a regimen of fludarabine 30 mg/m<sup>2</sup>/day × 5 days and Melphalan 140 mg/m<sup>2</sup> on day -1 (flu/Mel) followed by infusion of unmanipulated PBSC graft from a haploidentical donor. GVHD prophylaxis included cyclophosphamide 50 mg/kg/day on days 3 and 4, mycophenolate mofetil on day 35, and tacrolimus on day 180. Median age was 57 years (range from 35 to 68). Transplantation diagnosis included AML (<i>n</i> = 11), ALL (<i>n</i> = 4), MDS/MPD (<i>n</i> = 6), NHL/CLL (<i>n</i> = 3), and MM (<i>n</i> = 1). Using the refined Disease Risk Index (DRI), patients were low (<i>n</i> = 1), intermediate (<i>n</i> = 13), and high/very high (<i>n</i> = 11). 22 out of 25 patients engrafted with a median time to neutrophil and platelet engraftment of 18 days and 36 days, respectively. All engrafting patients achieved full peripheral blood T-lymphocyte and myeloid donor chimerism at day 30. The 180-day cumulative incidence for acute GVHD grades II-IV and III-IV was seen in 20% (95% CI 8%-37%) and 8% (95% CI 2%-22%), respectively. The 2-year cumulative incidence of chronic GVHD was 16% (95% CI 5%-33%) (moderate-severe 12% (95% CI 3%-27%)). After a median follow-up of 28.3 months, the estimated 2-year OS, DFS, NRM, and relapse were 56% (95%CI 33-74%), 44% (95%CI 23%-64%), 20% (95% CI 8%-37%), and 36% (95% CI 17%-55%), respectively. Among patients with high/very high risk DRI, 2-year OS was 53% compared to 69% for low/intermediate DRI. When compared with a contemporaneous cohort of patients at our center receiving haploidentical transplant with nonablative fludarabine, Cytoxan, and total body irradiation flu/Cy/TBI regimen, the outcomes were statistically similar to the 2-year OS at 56% vs. 63% <i>p</i>=0.75 and DFS at 44% vs. 46% <i>p</i>=0.65.</p>","PeriodicalId":7325,"journal":{"name":"Advances in Hematology","volume":"2021 ","pages":"8868142"},"PeriodicalIF":0.0000,"publicationDate":"2021-03-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8009703/pdf/","citationCount":"1","resultStr":"{\"title\":\"A Phase II Trial of Melphalan Based Reduced-Intensity Conditioning for Transplantation of T-Replete HLA-Haploidentical Peripheral Blood Stem Cells with Posttransplant Cyclophosphamide in Patients with Hematologic Malignancies.\",\"authors\":\"Melhem M Solh, Gabriel Hinojosa, Justin Laporte, Scott R Solomon, Lawrence E Morris, Xu Zhang, H Kent Holland, Asad Bashey\",\"doi\":\"10.1155/2021/8868142\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>T-replete haploidentical donor transplants using posttransplant cyclophosphamide (haplo) have greatly expanded donor availability and are increasingly utilized. Haplo were originally performed using truly nonmyeloablative conditioning and a bone marrow graft. We have also developed myeloablative conditioning and peripheral blood stem cell (PBSC) grafts for use with haplo. However, some patients may not tolerate myeloablative conditioning but may still benefit from a more dose-intensified preparative regimen to control malignancy and diminish graft rejection. To this end, we enrolled 25 patients on a prospective phase II trial utilizing a regimen of fludarabine 30 mg/m<sup>2</sup>/day × 5 days and Melphalan 140 mg/m<sup>2</sup> on day -1 (flu/Mel) followed by infusion of unmanipulated PBSC graft from a haploidentical donor. GVHD prophylaxis included cyclophosphamide 50 mg/kg/day on days 3 and 4, mycophenolate mofetil on day 35, and tacrolimus on day 180. Median age was 57 years (range from 35 to 68). Transplantation diagnosis included AML (<i>n</i> = 11), ALL (<i>n</i> = 4), MDS/MPD (<i>n</i> = 6), NHL/CLL (<i>n</i> = 3), and MM (<i>n</i> = 1). Using the refined Disease Risk Index (DRI), patients were low (<i>n</i> = 1), intermediate (<i>n</i> = 13), and high/very high (<i>n</i> = 11). 22 out of 25 patients engrafted with a median time to neutrophil and platelet engraftment of 18 days and 36 days, respectively. All engrafting patients achieved full peripheral blood T-lymphocyte and myeloid donor chimerism at day 30. The 180-day cumulative incidence for acute GVHD grades II-IV and III-IV was seen in 20% (95% CI 8%-37%) and 8% (95% CI 2%-22%), respectively. The 2-year cumulative incidence of chronic GVHD was 16% (95% CI 5%-33%) (moderate-severe 12% (95% CI 3%-27%)). After a median follow-up of 28.3 months, the estimated 2-year OS, DFS, NRM, and relapse were 56% (95%CI 33-74%), 44% (95%CI 23%-64%), 20% (95% CI 8%-37%), and 36% (95% CI 17%-55%), respectively. Among patients with high/very high risk DRI, 2-year OS was 53% compared to 69% for low/intermediate DRI. When compared with a contemporaneous cohort of patients at our center receiving haploidentical transplant with nonablative fludarabine, Cytoxan, and total body irradiation flu/Cy/TBI regimen, the outcomes were statistically similar to the 2-year OS at 56% vs. 63% <i>p</i>=0.75 and DFS at 44% vs. 46% <i>p</i>=0.65.</p>\",\"PeriodicalId\":7325,\"journal\":{\"name\":\"Advances in Hematology\",\"volume\":\"2021 \",\"pages\":\"8868142\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-03-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8009703/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Advances in Hematology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2021/8868142\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Advances in Hematology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/8868142","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
摘要
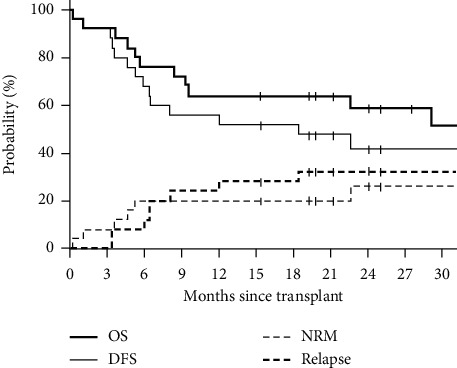
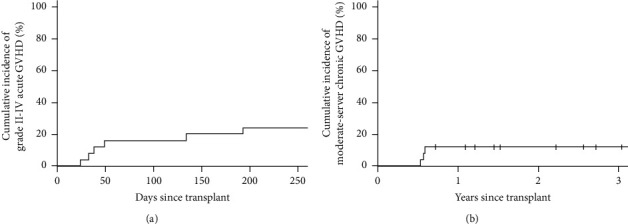
使用移植后环磷酰胺(haplo)的t -满单倍体同种供体移植极大地扩大了供体的可用性,并且越来越多地被利用。Haplo最初是使用真正的非清髓性条件和骨髓移植进行的。我们还开发了用于单倍体的清髓调节和外周血干细胞(PBSC)移植。然而,一些患者可能不能耐受清髓调节,但可能仍然受益于更大剂量强化的预备方案,以控制恶性肿瘤和减少移植排斥。为此,我们招募了25名患者进行前瞻性II期试验,使用氟达拉滨30 mg/m2/天× 5天,美法兰140 mg/m2,第1天(流感/梅尔),然后输注来自单倍体相同供体的未经处理的PBSC移植物。GVHD预防包括环磷酰胺50 mg/kg/天(第3天和第4天)、霉酚酸酯(第35天)和他克莫司(第180天)。中位年龄为57岁(35 - 68岁)。移植诊断包括AML (n = 11)、ALL (n = 4)、MDS/MPD (n = 6)、NHL/CLL (n = 3)、MM (n = 1)。使用改进的疾病风险指数(DRI),患者分为低(n = 1)、中(n = 13)和高/非常高(n = 11)。25例患者中有22例移植到中性粒细胞和血小板的中位时间分别为18天和36天。所有移植患者在第30天外周血t淋巴细胞和骨髓供体完全嵌合。急性GVHD II-IV级和III-IV级的180天累积发病率分别为20% (95% CI 8%-37%)和8% (95% CI 2%-22%)。慢性GVHD的2年累积发病率为16% (95% CI 5%-33%)(中重度12% (95% CI 3%-27%))。中位随访28.3个月后,估计2年OS、DFS、NRM和复发率分别为56% (95%CI 33-74%)、44% (95%CI 23%-64%)、20% (95%CI 8%-37%)和36% (95%CI 17%-55%)。在高/非常高风险DRI患者中,2年OS为53%,而低/中度DRI患者为69%。与本中心同期接受单倍体移植的非消融性氟达拉滨、环磷酰胺和全身照射流感/Cy/TBI方案的患者进行比较,结果与2年OS (56% vs. 63% p=0.75)和DFS (44% vs. 46% p=0.65)在统计学上相似。
A Phase II Trial of Melphalan Based Reduced-Intensity Conditioning for Transplantation of T-Replete HLA-Haploidentical Peripheral Blood Stem Cells with Posttransplant Cyclophosphamide in Patients with Hematologic Malignancies.
T-replete haploidentical donor transplants using posttransplant cyclophosphamide (haplo) have greatly expanded donor availability and are increasingly utilized. Haplo were originally performed using truly nonmyeloablative conditioning and a bone marrow graft. We have also developed myeloablative conditioning and peripheral blood stem cell (PBSC) grafts for use with haplo. However, some patients may not tolerate myeloablative conditioning but may still benefit from a more dose-intensified preparative regimen to control malignancy and diminish graft rejection. To this end, we enrolled 25 patients on a prospective phase II trial utilizing a regimen of fludarabine 30 mg/m2/day × 5 days and Melphalan 140 mg/m2 on day -1 (flu/Mel) followed by infusion of unmanipulated PBSC graft from a haploidentical donor. GVHD prophylaxis included cyclophosphamide 50 mg/kg/day on days 3 and 4, mycophenolate mofetil on day 35, and tacrolimus on day 180. Median age was 57 years (range from 35 to 68). Transplantation diagnosis included AML (n = 11), ALL (n = 4), MDS/MPD (n = 6), NHL/CLL (n = 3), and MM (n = 1). Using the refined Disease Risk Index (DRI), patients were low (n = 1), intermediate (n = 13), and high/very high (n = 11). 22 out of 25 patients engrafted with a median time to neutrophil and platelet engraftment of 18 days and 36 days, respectively. All engrafting patients achieved full peripheral blood T-lymphocyte and myeloid donor chimerism at day 30. The 180-day cumulative incidence for acute GVHD grades II-IV and III-IV was seen in 20% (95% CI 8%-37%) and 8% (95% CI 2%-22%), respectively. The 2-year cumulative incidence of chronic GVHD was 16% (95% CI 5%-33%) (moderate-severe 12% (95% CI 3%-27%)). After a median follow-up of 28.3 months, the estimated 2-year OS, DFS, NRM, and relapse were 56% (95%CI 33-74%), 44% (95%CI 23%-64%), 20% (95% CI 8%-37%), and 36% (95% CI 17%-55%), respectively. Among patients with high/very high risk DRI, 2-year OS was 53% compared to 69% for low/intermediate DRI. When compared with a contemporaneous cohort of patients at our center receiving haploidentical transplant with nonablative fludarabine, Cytoxan, and total body irradiation flu/Cy/TBI regimen, the outcomes were statistically similar to the 2-year OS at 56% vs. 63% p=0.75 and DFS at 44% vs. 46% p=0.65.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
