Cirous Sadeghi, Hassan A. Khan, Gregory Gudleski, Jessica L. Reynolds, Smita Y. Bakhai
{"title":"改善初级保健诊所血压控制的多方面策略:一个质量改进项目","authors":"Cirous Sadeghi, Hassan A. Khan, Gregory Gudleski, Jessica L. Reynolds, Smita Y. Bakhai","doi":"10.1016/j.ijchy.2020.100060","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Approximately 80% of patients with hypertension in the Internal Medicine Clinic were uncontrolled (BP > 130/80 mmHg), according to the 2017 American College of Cardiology (ACC)/American Heart Association (AHA) hypertension guidelines, leading to increased morbidity and mortality. The aim of this quality improvement (QI) was to improve BP control <130/80 from the baseline rates of 20%–30% and <140/90 from the baseline rates of 40%–60% between ages of 18–75 years, within 12 months.</p></div><div><h3>Methods</h3><p>We used the Plan-Do-Study-Act method. A multidisciplinary QI team identified barriers by fish bone diagram. Barriers included: 1) Physicians' knowledge gap and clinical inertia in optimization of medications, and 2) Patients' nonadherence to medication and appointments. The outcome measures were the percentage of patients with BP < 140/90 and < 130/80. Process measures included: 1) attendance rates of physician and nurses at educational sessions, 2) medication reconciliation completion rates and 3) care guide order rates. Key interventions were: 1) physicians and nurses' education regarding ACC/AHA guidelines, 2) patient education and engagement and 3) enhancement of health information technology. Data analysis was performed using monthly statistical process control charts.</p></div><div><h3>Results</h3><p>We achieved 62.6% (n = 885/1426) for BP < 140/90 and 24.47% (n = 349/1426) for BP < 130/80 within 12 months project period. We sustained and exceeded at 72.64% (n = 945/1301) for BP < 140/90 and 44.58% (n = 580/1301) for BP < 130/80 during the 10 months post-project period.</p></div><div><h3>Conclusions</h3><p>Overcoming physician clinical inertia, enhancing patient adherence to appointments and medications, and a high functioning multidisciplinary team were the key drivers for the success.</p></div>","PeriodicalId":36839,"journal":{"name":"International Journal of Cardiology: Hypertension","volume":"7 ","pages":"Article 100060"},"PeriodicalIF":0.0000,"publicationDate":"2020-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.ijchy.2020.100060","citationCount":"8","resultStr":"{\"title\":\"Multifaceted strategies to improve blood pressure control in a primary care clinic: A quality improvement project\",\"authors\":\"Cirous Sadeghi, Hassan A. Khan, Gregory Gudleski, Jessica L. Reynolds, Smita Y. Bakhai\",\"doi\":\"10.1016/j.ijchy.2020.100060\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Approximately 80% of patients with hypertension in the Internal Medicine Clinic were uncontrolled (BP > 130/80 mmHg), according to the 2017 American College of Cardiology (ACC)/American Heart Association (AHA) hypertension guidelines, leading to increased morbidity and mortality. The aim of this quality improvement (QI) was to improve BP control <130/80 from the baseline rates of 20%–30% and <140/90 from the baseline rates of 40%–60% between ages of 18–75 years, within 12 months.</p></div><div><h3>Methods</h3><p>We used the Plan-Do-Study-Act method. A multidisciplinary QI team identified barriers by fish bone diagram. Barriers included: 1) Physicians' knowledge gap and clinical inertia in optimization of medications, and 2) Patients' nonadherence to medication and appointments. The outcome measures were the percentage of patients with BP < 140/90 and < 130/80. Process measures included: 1) attendance rates of physician and nurses at educational sessions, 2) medication reconciliation completion rates and 3) care guide order rates. Key interventions were: 1) physicians and nurses' education regarding ACC/AHA guidelines, 2) patient education and engagement and 3) enhancement of health information technology. Data analysis was performed using monthly statistical process control charts.</p></div><div><h3>Results</h3><p>We achieved 62.6% (n = 885/1426) for BP < 140/90 and 24.47% (n = 349/1426) for BP < 130/80 within 12 months project period. We sustained and exceeded at 72.64% (n = 945/1301) for BP < 140/90 and 44.58% (n = 580/1301) for BP < 130/80 during the 10 months post-project period.</p></div><div><h3>Conclusions</h3><p>Overcoming physician clinical inertia, enhancing patient adherence to appointments and medications, and a high functioning multidisciplinary team were the key drivers for the success.</p></div>\",\"PeriodicalId\":36839,\"journal\":{\"name\":\"International Journal of Cardiology: Hypertension\",\"volume\":\"7 \",\"pages\":\"Article 100060\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1016/j.ijchy.2020.100060\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Cardiology: Hypertension\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2590086220300379\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/10/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Cardiology: Hypertension","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590086220300379","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/10/27 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Multifaceted strategies to improve blood pressure control in a primary care clinic: A quality improvement project
Background
Approximately 80% of patients with hypertension in the Internal Medicine Clinic were uncontrolled (BP > 130/80 mmHg), according to the 2017 American College of Cardiology (ACC)/American Heart Association (AHA) hypertension guidelines, leading to increased morbidity and mortality. The aim of this quality improvement (QI) was to improve BP control <130/80 from the baseline rates of 20%–30% and <140/90 from the baseline rates of 40%–60% between ages of 18–75 years, within 12 months.
Methods
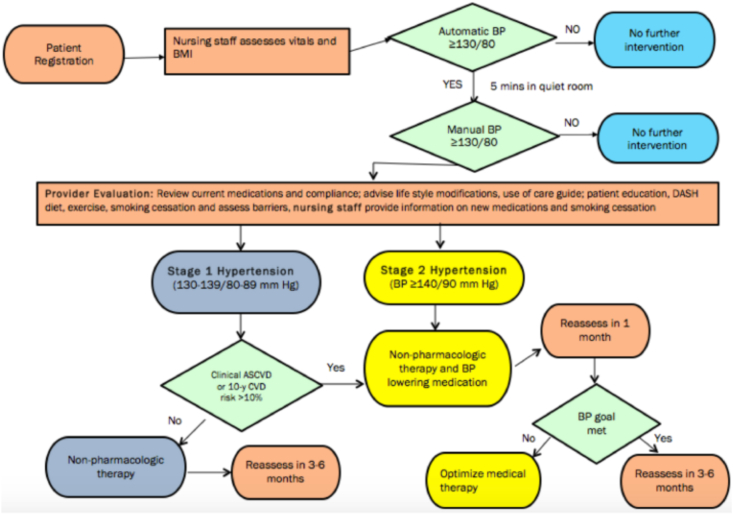
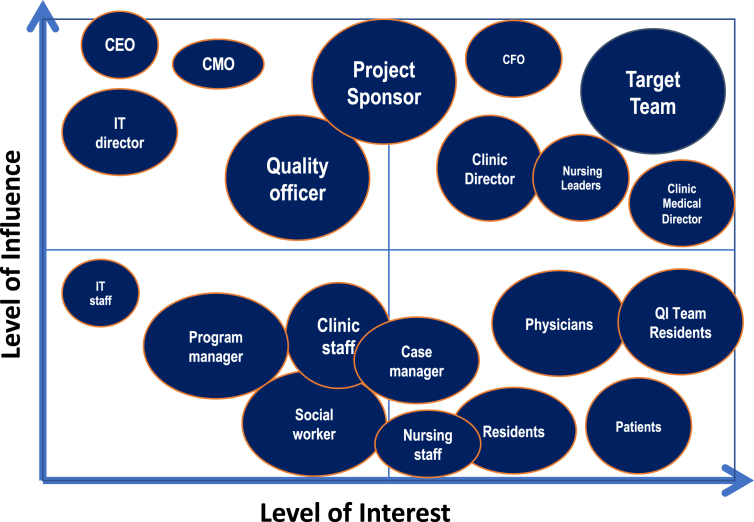
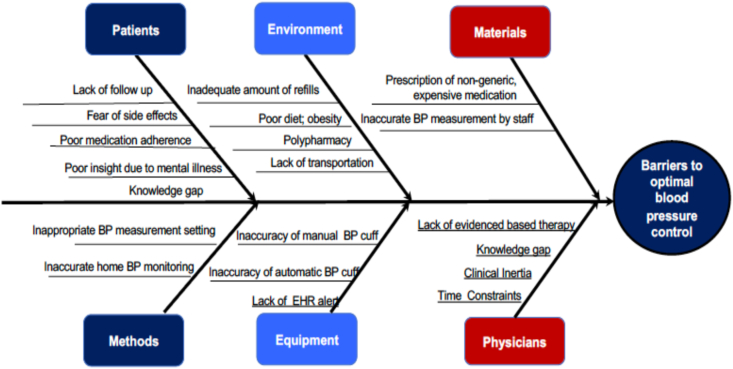
We used the Plan-Do-Study-Act method. A multidisciplinary QI team identified barriers by fish bone diagram. Barriers included: 1) Physicians' knowledge gap and clinical inertia in optimization of medications, and 2) Patients' nonadherence to medication and appointments. The outcome measures were the percentage of patients with BP < 140/90 and < 130/80. Process measures included: 1) attendance rates of physician and nurses at educational sessions, 2) medication reconciliation completion rates and 3) care guide order rates. Key interventions were: 1) physicians and nurses' education regarding ACC/AHA guidelines, 2) patient education and engagement and 3) enhancement of health information technology. Data analysis was performed using monthly statistical process control charts.
Results
We achieved 62.6% (n = 885/1426) for BP < 140/90 and 24.47% (n = 349/1426) for BP < 130/80 within 12 months project period. We sustained and exceeded at 72.64% (n = 945/1301) for BP < 140/90 and 44.58% (n = 580/1301) for BP < 130/80 during the 10 months post-project period.
Conclusions
Overcoming physician clinical inertia, enhancing patient adherence to appointments and medications, and a high functioning multidisciplinary team were the key drivers for the success.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
