Markus Heim, Tobias Lahmer, Sebastian Rasch, Silja Kriescher, Wiebke Berg-Johnson, Kristina Fuest, Barbara Kapfer, Gerhard Schneider, Christoph D Spinner, Fabian Geisler, Johannes R Wießner, Kathrin Rothe, Susanne Feihl, Andreas Ranft
{"title":"一份初步报告:COVID-19的快速临床演变导致早期住院和不利结果","authors":"Markus Heim, Tobias Lahmer, Sebastian Rasch, Silja Kriescher, Wiebke Berg-Johnson, Kristina Fuest, Barbara Kapfer, Gerhard Schneider, Christoph D Spinner, Fabian Geisler, Johannes R Wießner, Kathrin Rothe, Susanne Feihl, Andreas Ranft","doi":"10.4081/mrm.2021.744","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A wide range of mortality rates has been reported in COVID-19 patients on the intensive care unit. We wanted to describe the clinical course and determine the mortality rate in our institution's intensive care units.</p><p><strong>Methods: </strong>To this end, we performed a retrospective cohort study of 50 COVID-19 patients admitted to the ICU at a large German tertiary university hospital. Clinical features are reported with a focus on ICU interventions, such as mechanical ventilation, prone positioning and extracorporeal organ support. Outcome is presented using a 7-point ordinal scale on day 28 and 60 following ICU admission.</p><p><strong>Results: </strong>The median age was 64 years, 78% were male. LDH and D-Dimers were elevated, and patients were low on Vitamin D. ARDS incidence was 75%, and 43/50 patients needed invasive ventilation. 22/50 patients intermittently needed prone positioning, and 7/50 required ECMO. The interval from onset of the first symptoms to admission to the hospital and to the ICU was shorter in non-survivors than in survivors. By day 60 after ICU admission, 52% of the patients had been discharged. 60-day mortality rate was 32%; 37% for ventilated patients, and 42% for those requiring both: ventilation and renal replacement therapy.</p><p><strong>Conclusions: </strong>Early deterioration might be seen as a warning signal for unfavourable outcome. Lung-protective ventilation including prone positioning remain the mainstay of the treatment.</p>","PeriodicalId":49031,"journal":{"name":"Multidisciplinary Respiratory Medicine","volume":"16 1","pages":"744"},"PeriodicalIF":1.6000,"publicationDate":"2021-04-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/66/6a/mrm-16-1-744.PMC8056325.pdf","citationCount":"0","resultStr":"{\"title\":\"Rapid clinical evolution for COVID-19 translates into early hospital admission and unfavourable outcome: a preliminary report.\",\"authors\":\"Markus Heim, Tobias Lahmer, Sebastian Rasch, Silja Kriescher, Wiebke Berg-Johnson, Kristina Fuest, Barbara Kapfer, Gerhard Schneider, Christoph D Spinner, Fabian Geisler, Johannes R Wießner, Kathrin Rothe, Susanne Feihl, Andreas Ranft\",\"doi\":\"10.4081/mrm.2021.744\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A wide range of mortality rates has been reported in COVID-19 patients on the intensive care unit. We wanted to describe the clinical course and determine the mortality rate in our institution's intensive care units.</p><p><strong>Methods: </strong>To this end, we performed a retrospective cohort study of 50 COVID-19 patients admitted to the ICU at a large German tertiary university hospital. Clinical features are reported with a focus on ICU interventions, such as mechanical ventilation, prone positioning and extracorporeal organ support. Outcome is presented using a 7-point ordinal scale on day 28 and 60 following ICU admission.</p><p><strong>Results: </strong>The median age was 64 years, 78% were male. LDH and D-Dimers were elevated, and patients were low on Vitamin D. ARDS incidence was 75%, and 43/50 patients needed invasive ventilation. 22/50 patients intermittently needed prone positioning, and 7/50 required ECMO. The interval from onset of the first symptoms to admission to the hospital and to the ICU was shorter in non-survivors than in survivors. By day 60 after ICU admission, 52% of the patients had been discharged. 60-day mortality rate was 32%; 37% for ventilated patients, and 42% for those requiring both: ventilation and renal replacement therapy.</p><p><strong>Conclusions: </strong>Early deterioration might be seen as a warning signal for unfavourable outcome. Lung-protective ventilation including prone positioning remain the mainstay of the treatment.</p>\",\"PeriodicalId\":49031,\"journal\":{\"name\":\"Multidisciplinary Respiratory Medicine\",\"volume\":\"16 1\",\"pages\":\"744\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2021-04-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/66/6a/mrm-16-1-744.PMC8056325.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Multidisciplinary Respiratory Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4081/mrm.2021.744\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/15 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Multidisciplinary Respiratory Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4081/mrm.2021.744","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/15 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Rapid clinical evolution for COVID-19 translates into early hospital admission and unfavourable outcome: a preliminary report.
Background: A wide range of mortality rates has been reported in COVID-19 patients on the intensive care unit. We wanted to describe the clinical course and determine the mortality rate in our institution's intensive care units.
Methods: To this end, we performed a retrospective cohort study of 50 COVID-19 patients admitted to the ICU at a large German tertiary university hospital. Clinical features are reported with a focus on ICU interventions, such as mechanical ventilation, prone positioning and extracorporeal organ support. Outcome is presented using a 7-point ordinal scale on day 28 and 60 following ICU admission.
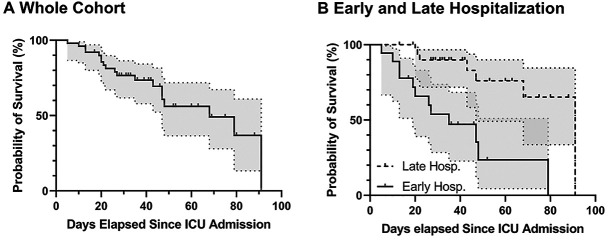
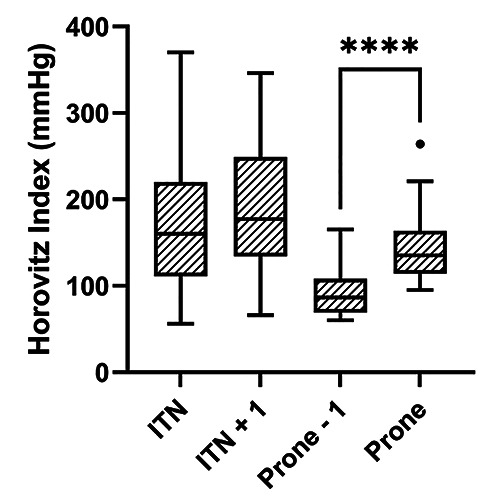
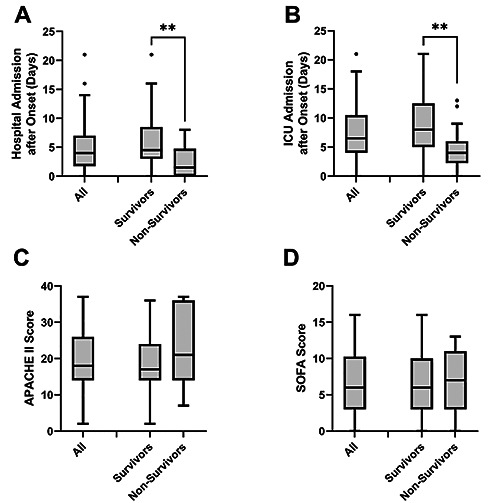
Results: The median age was 64 years, 78% were male. LDH and D-Dimers were elevated, and patients were low on Vitamin D. ARDS incidence was 75%, and 43/50 patients needed invasive ventilation. 22/50 patients intermittently needed prone positioning, and 7/50 required ECMO. The interval from onset of the first symptoms to admission to the hospital and to the ICU was shorter in non-survivors than in survivors. By day 60 after ICU admission, 52% of the patients had been discharged. 60-day mortality rate was 32%; 37% for ventilated patients, and 42% for those requiring both: ventilation and renal replacement therapy.
Conclusions: Early deterioration might be seen as a warning signal for unfavourable outcome. Lung-protective ventilation including prone positioning remain the mainstay of the treatment.
期刊介绍:
Multidisciplinary Respiratory Medicine is the official journal of the Italian Respiratory Society - Società Italiana di Pneumologia (IRS/SIP). The journal publishes on all aspects of respiratory medicine and related fields, with a particular focus on interdisciplinary and translational research.
The interdisciplinary nature of the journal provides a unique opportunity for researchers, clinicians and healthcare professionals across specialties to collaborate and exchange information. The journal provides a high visibility platform for the publication and dissemination of top quality original scientific articles, reviews and important position papers documenting clinical and experimental advances.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
