Vildan Koc, Laura Delmas Benito, Eldert de With, E Christiaan Boerma
{"title":"液体负荷对心脏手术后可归因发病率的影响:一项回顾性研究。","authors":"Vildan Koc, Laura Delmas Benito, Eldert de With, E Christiaan Boerma","doi":"10.1155/2020/4836862","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Although the detrimental effects of excessive perioperative fluid administration are generally well established, data in the setting of cardiac surgery remain less robust.</p><p><strong>Methods: </strong>In this retrospective single-center observational study, the total fluid balance in the first 12 hours during and after surgery was evaluated. Primary endpoint was the relationship between total fluid balance and the incidence of prolonged mechanical ventilation. For this purpose, data were divided into quartiles (Q); prolonged mechanical ventilation and prolonged length of stay (LOS) in the ICU were defined as Q4. Secondary endpoints were prolonged LOS in the ICU, incidence of acute kidney injury (AKI; defined as a 1.5-fold increase in serum creatinine during, relative to baseline), and ICU mortality.</p><p><strong>Results: </strong>In a 3-year period, 748 patients were included. In a univariate analysis, the median duration of mechanical ventilation was 2.9 h [2.4-3.7] in Q1 of the fluid balance and increased significantly to 4.7 h [3.1-9.2] in Q4 of the fluid balance (<i>p</i> < 0.001). In addition, patients in Q4 of the fluid balance had a significantly longer LOS in the ICU, as well as a higher incidence of AKI and ICU mortality. In a multivariate analysis, Q4 of the fluid balance was independently associated with prolonged mechanical ventilation (OR 4.9, CI 2.9-8.4, <i>p</i> < 0.001) and prolonged LOS in the ICU (OR 11.3 CI 6.1-20,9, <i>p</i> < 0.001), but not with the incidence of AKI or ICU mortality.</p><p><strong>Conclusions: </strong>Perioperative fluid administration in cardiac surgery patients was independently associated with prolonged mechanical ventilation and prolonged LOS in the ICU.</p>","PeriodicalId":46583,"journal":{"name":"Critical Care Research and Practice","volume":"2020 ","pages":"4836862"},"PeriodicalIF":1.8000,"publicationDate":"2020-12-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/4836862","citationCount":"7","resultStr":"{\"title\":\"The Effect of Fluid Overload on Attributable Morbidity after Cardiac Surgery: A Retrospective Study.\",\"authors\":\"Vildan Koc, Laura Delmas Benito, Eldert de With, E Christiaan Boerma\",\"doi\":\"10.1155/2020/4836862\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Although the detrimental effects of excessive perioperative fluid administration are generally well established, data in the setting of cardiac surgery remain less robust.</p><p><strong>Methods: </strong>In this retrospective single-center observational study, the total fluid balance in the first 12 hours during and after surgery was evaluated. Primary endpoint was the relationship between total fluid balance and the incidence of prolonged mechanical ventilation. For this purpose, data were divided into quartiles (Q); prolonged mechanical ventilation and prolonged length of stay (LOS) in the ICU were defined as Q4. Secondary endpoints were prolonged LOS in the ICU, incidence of acute kidney injury (AKI; defined as a 1.5-fold increase in serum creatinine during, relative to baseline), and ICU mortality.</p><p><strong>Results: </strong>In a 3-year period, 748 patients were included. In a univariate analysis, the median duration of mechanical ventilation was 2.9 h [2.4-3.7] in Q1 of the fluid balance and increased significantly to 4.7 h [3.1-9.2] in Q4 of the fluid balance (<i>p</i> < 0.001). In addition, patients in Q4 of the fluid balance had a significantly longer LOS in the ICU, as well as a higher incidence of AKI and ICU mortality. In a multivariate analysis, Q4 of the fluid balance was independently associated with prolonged mechanical ventilation (OR 4.9, CI 2.9-8.4, <i>p</i> < 0.001) and prolonged LOS in the ICU (OR 11.3 CI 6.1-20,9, <i>p</i> < 0.001), but not with the incidence of AKI or ICU mortality.</p><p><strong>Conclusions: </strong>Perioperative fluid administration in cardiac surgery patients was independently associated with prolonged mechanical ventilation and prolonged LOS in the ICU.</p>\",\"PeriodicalId\":46583,\"journal\":{\"name\":\"Critical Care Research and Practice\",\"volume\":\"2020 \",\"pages\":\"4836862\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2020-12-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2020/4836862\",\"citationCount\":\"7\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Critical Care Research and Practice\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2020/4836862\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CRITICAL CARE MEDICINE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care Research and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/4836862","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 7
摘要
导论:虽然围手术期过量输液的有害影响通常是公认的,但在心脏手术方面的数据仍然不那么可靠。方法:在这项回顾性单中心观察研究中,评估手术中和术后前12小时的总体液平衡。主要终点是总体液平衡与延长机械通气发生率之间的关系。为此,将数据分成四分位数(Q);延长机械通气时间和延长ICU住院时间(LOS)被定义为Q4。次要终点是ICU中延长的LOS,急性肾损伤(AKI)的发生率;定义为与基线相比血清肌酐升高1.5倍)和ICU死亡率。结果:在3年的时间里,纳入了748例患者。在单因素分析中,第一季度机械通气的中位持续时间为2.9 h[2.4-3.7],第4季度机械通气的中位持续时间显著增加至4.7 h [3.1-9.2] (p < 0.001)。此外,体液平衡Q4的患者在ICU的LOS明显更长,AKI发生率和ICU死亡率也更高。在一项多变量分析中,体液平衡的Q4与延长机械通气时间(OR 4.9, CI 2.9-8.4, p < 0.001)和延长ICU内的LOS (OR 11.3, CI 6.1-20,9, p < 0.001)独立相关,但与AKI发生率或ICU死亡率无关。结论:心脏手术患者围手术期输液与ICU机械通气时间延长和LOS延长独立相关。
The Effect of Fluid Overload on Attributable Morbidity after Cardiac Surgery: A Retrospective Study.
Introduction: Although the detrimental effects of excessive perioperative fluid administration are generally well established, data in the setting of cardiac surgery remain less robust.
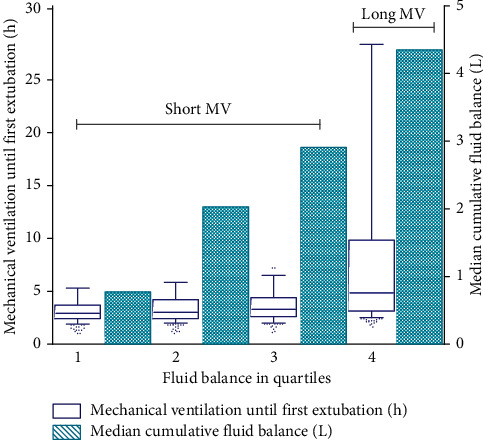
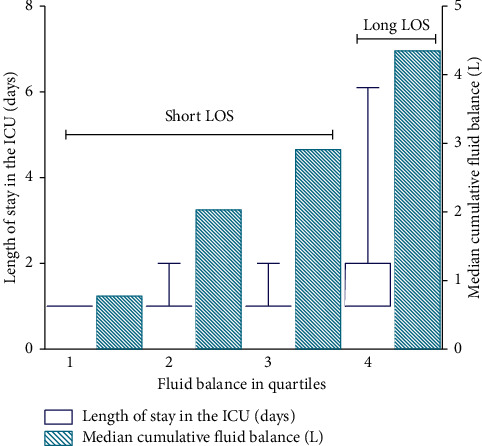
Methods: In this retrospective single-center observational study, the total fluid balance in the first 12 hours during and after surgery was evaluated. Primary endpoint was the relationship between total fluid balance and the incidence of prolonged mechanical ventilation. For this purpose, data were divided into quartiles (Q); prolonged mechanical ventilation and prolonged length of stay (LOS) in the ICU were defined as Q4. Secondary endpoints were prolonged LOS in the ICU, incidence of acute kidney injury (AKI; defined as a 1.5-fold increase in serum creatinine during, relative to baseline), and ICU mortality.
Results: In a 3-year period, 748 patients were included. In a univariate analysis, the median duration of mechanical ventilation was 2.9 h [2.4-3.7] in Q1 of the fluid balance and increased significantly to 4.7 h [3.1-9.2] in Q4 of the fluid balance (p < 0.001). In addition, patients in Q4 of the fluid balance had a significantly longer LOS in the ICU, as well as a higher incidence of AKI and ICU mortality. In a multivariate analysis, Q4 of the fluid balance was independently associated with prolonged mechanical ventilation (OR 4.9, CI 2.9-8.4, p < 0.001) and prolonged LOS in the ICU (OR 11.3 CI 6.1-20,9, p < 0.001), but not with the incidence of AKI or ICU mortality.
Conclusions: Perioperative fluid administration in cardiac surgery patients was independently associated with prolonged mechanical ventilation and prolonged LOS in the ICU.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
