Rebecca J Baer, Nichole Nidey, Gretchen Bandoli, Brittany D Chambers, Christina D Chambers, Sky Feuer, Deborah Karasek, Scott P Oltman, Larry Rand, Kelli K Ryckman, Laura L Jelliffe-Pawlowski
{"title":"尿路感染妇女早产的风险:一项回顾性队列研究","authors":"Rebecca J Baer, Nichole Nidey, Gretchen Bandoli, Brittany D Chambers, Christina D Chambers, Sky Feuer, Deborah Karasek, Scott P Oltman, Larry Rand, Kelli K Ryckman, Laura L Jelliffe-Pawlowski","doi":"10.1055/s-0040-1721668","DOIUrl":null,"url":null,"abstract":"<p><p><b>Objective</b> The aim of the study is to evaluate the risk of preterm birth (PTB, <37 weeks) and early term (37 and 38 weeks) birth among women with an emergency department (ED) visit or hospitalization with a urinary tract infection (UTI) by trimester of pregnancy. <b>Methods</b> The primary sample was selected from births in California between 2011 and 2017. UTIs were identified from the ED or hospital discharge records. Risk of PTB, by subtype, and early term birth were evaluated by trimester of pregnancy and by type of visit using log-linear regression. Risk ratios were adjusted for maternal factors. Antibiotic usage was examined in a population of privately insured women from Iowa. <b>Results</b> Women with a UTI during pregnancy were at elevated risk of a birth <32 weeks, 32 to 36 weeks, and 37 to 38 weeks (adjusted risk ratios [aRRs] 1.1-1.4). Of the women with a diagnostic code for multiple bacterial species, 28.8% had a PTB. A UTI diagnosis elevated risk of PTB regardless of antibiotic treatment (aRR 1.4 for treated, aRR 1.5 for untreated). <b>Conclusion</b> UTIs are associated with early birth. This association is present regardless of the trimester of pregnancy, type of PTB, and antibiotic treatment.</p>","PeriodicalId":7645,"journal":{"name":"AJP Reports","volume":"11 1","pages":"e5-e14"},"PeriodicalIF":0.6000,"publicationDate":"2021-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1055/s-0040-1721668","citationCount":"8","resultStr":"{\"title\":\"Risk of Early Birth among Women with a Urinary Tract Infection: A Retrospective Cohort Study.\",\"authors\":\"Rebecca J Baer, Nichole Nidey, Gretchen Bandoli, Brittany D Chambers, Christina D Chambers, Sky Feuer, Deborah Karasek, Scott P Oltman, Larry Rand, Kelli K Ryckman, Laura L Jelliffe-Pawlowski\",\"doi\":\"10.1055/s-0040-1721668\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Objective</b> The aim of the study is to evaluate the risk of preterm birth (PTB, <37 weeks) and early term (37 and 38 weeks) birth among women with an emergency department (ED) visit or hospitalization with a urinary tract infection (UTI) by trimester of pregnancy. <b>Methods</b> The primary sample was selected from births in California between 2011 and 2017. UTIs were identified from the ED or hospital discharge records. Risk of PTB, by subtype, and early term birth were evaluated by trimester of pregnancy and by type of visit using log-linear regression. Risk ratios were adjusted for maternal factors. Antibiotic usage was examined in a population of privately insured women from Iowa. <b>Results</b> Women with a UTI during pregnancy were at elevated risk of a birth <32 weeks, 32 to 36 weeks, and 37 to 38 weeks (adjusted risk ratios [aRRs] 1.1-1.4). Of the women with a diagnostic code for multiple bacterial species, 28.8% had a PTB. A UTI diagnosis elevated risk of PTB regardless of antibiotic treatment (aRR 1.4 for treated, aRR 1.5 for untreated). <b>Conclusion</b> UTIs are associated with early birth. This association is present regardless of the trimester of pregnancy, type of PTB, and antibiotic treatment.</p>\",\"PeriodicalId\":7645,\"journal\":{\"name\":\"AJP Reports\",\"volume\":\"11 1\",\"pages\":\"e5-e14\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2021-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1055/s-0040-1721668\",\"citationCount\":\"8\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"AJP Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1055/s-0040-1721668\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/13 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"PEDIATRICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"AJP Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0040-1721668","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/13 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"PEDIATRICS","Score":null,"Total":0}
Risk of Early Birth among Women with a Urinary Tract Infection: A Retrospective Cohort Study.
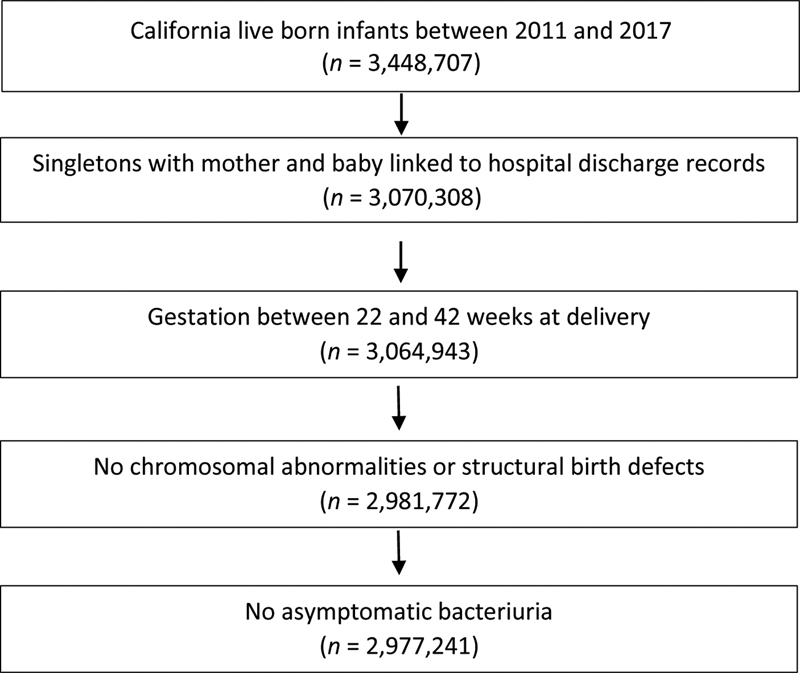
Objective The aim of the study is to evaluate the risk of preterm birth (PTB, <37 weeks) and early term (37 and 38 weeks) birth among women with an emergency department (ED) visit or hospitalization with a urinary tract infection (UTI) by trimester of pregnancy. Methods The primary sample was selected from births in California between 2011 and 2017. UTIs were identified from the ED or hospital discharge records. Risk of PTB, by subtype, and early term birth were evaluated by trimester of pregnancy and by type of visit using log-linear regression. Risk ratios were adjusted for maternal factors. Antibiotic usage was examined in a population of privately insured women from Iowa. Results Women with a UTI during pregnancy were at elevated risk of a birth <32 weeks, 32 to 36 weeks, and 37 to 38 weeks (adjusted risk ratios [aRRs] 1.1-1.4). Of the women with a diagnostic code for multiple bacterial species, 28.8% had a PTB. A UTI diagnosis elevated risk of PTB regardless of antibiotic treatment (aRR 1.4 for treated, aRR 1.5 for untreated). Conclusion UTIs are associated with early birth. This association is present regardless of the trimester of pregnancy, type of PTB, and antibiotic treatment.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
