Macaulay Amechi Onuigbo, Heng Tan, Sarah E Sherman
{"title":"成人镰状细胞病交替和并发的真高钾血症和假高钾血症。","authors":"Macaulay Amechi Onuigbo, Heng Tan, Sarah E Sherman","doi":"10.5041/RMMJ.10439","DOIUrl":null,"url":null,"abstract":"<p><p>Sickle cell disease (SCD) predisposes the patient to recurrent episodes of acute painful hemolytic crisis. Sickle cell nephropathy (SCN) is not uncommon in adult patients, and renal manifestations of SCN include renal ischemia, microinfarcts, renal papillary necrosis, and renal tubular abnormalities with variable clinical presentations. Intravascular hemolysis and reduced glomerular filtration rate with renal tubular dysfunction predispose to true hyperkalemia. Hemolytic crisis can be complicated by sepsis, leading to significant degrees of thrombocytosis, and thrombocytosis is a well-defined cause of pseudohyperkalemia. We describe a 40-year-old African American male patient with sickle cell anemia who exhibited alternating episodes of true hyperkalemia and pseudohyperkalemia, during consecutive hospital admissions. Clearly, true hyperkalemia is a potentially lethal condition. At the same time, the institution of inappropriate and intensive treatment of pseudohyperkalemia leading to severe hypokalemia is also potentially lethal. The need for this caution is most imperative with the recent introduction of the safer and more potent potassium binders, patiromer and sodium zirconium cyclosilicate.</p>","PeriodicalId":46408,"journal":{"name":"Rambam Maimonides Medical Journal","volume":"12 2","pages":""},"PeriodicalIF":1.3000,"publicationDate":"2021-04-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8092952/pdf/","citationCount":"1","resultStr":"{\"title\":\"Alternating and Concurrent True Hyperkalemia and Pseudohyperkalemia in Adult Sickle Cell Disease.\",\"authors\":\"Macaulay Amechi Onuigbo, Heng Tan, Sarah E Sherman\",\"doi\":\"10.5041/RMMJ.10439\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Sickle cell disease (SCD) predisposes the patient to recurrent episodes of acute painful hemolytic crisis. Sickle cell nephropathy (SCN) is not uncommon in adult patients, and renal manifestations of SCN include renal ischemia, microinfarcts, renal papillary necrosis, and renal tubular abnormalities with variable clinical presentations. Intravascular hemolysis and reduced glomerular filtration rate with renal tubular dysfunction predispose to true hyperkalemia. Hemolytic crisis can be complicated by sepsis, leading to significant degrees of thrombocytosis, and thrombocytosis is a well-defined cause of pseudohyperkalemia. We describe a 40-year-old African American male patient with sickle cell anemia who exhibited alternating episodes of true hyperkalemia and pseudohyperkalemia, during consecutive hospital admissions. Clearly, true hyperkalemia is a potentially lethal condition. At the same time, the institution of inappropriate and intensive treatment of pseudohyperkalemia leading to severe hypokalemia is also potentially lethal. The need for this caution is most imperative with the recent introduction of the safer and more potent potassium binders, patiromer and sodium zirconium cyclosilicate.</p>\",\"PeriodicalId\":46408,\"journal\":{\"name\":\"Rambam Maimonides Medical Journal\",\"volume\":\"12 2\",\"pages\":\"\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2021-04-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8092952/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Rambam Maimonides Medical Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5041/RMMJ.10439\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Rambam Maimonides Medical Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5041/RMMJ.10439","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Alternating and Concurrent True Hyperkalemia and Pseudohyperkalemia in Adult Sickle Cell Disease.
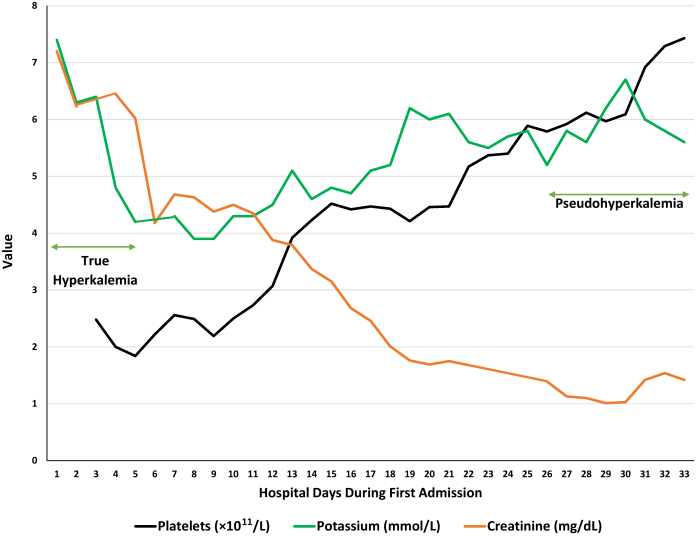
Sickle cell disease (SCD) predisposes the patient to recurrent episodes of acute painful hemolytic crisis. Sickle cell nephropathy (SCN) is not uncommon in adult patients, and renal manifestations of SCN include renal ischemia, microinfarcts, renal papillary necrosis, and renal tubular abnormalities with variable clinical presentations. Intravascular hemolysis and reduced glomerular filtration rate with renal tubular dysfunction predispose to true hyperkalemia. Hemolytic crisis can be complicated by sepsis, leading to significant degrees of thrombocytosis, and thrombocytosis is a well-defined cause of pseudohyperkalemia. We describe a 40-year-old African American male patient with sickle cell anemia who exhibited alternating episodes of true hyperkalemia and pseudohyperkalemia, during consecutive hospital admissions. Clearly, true hyperkalemia is a potentially lethal condition. At the same time, the institution of inappropriate and intensive treatment of pseudohyperkalemia leading to severe hypokalemia is also potentially lethal. The need for this caution is most imperative with the recent introduction of the safer and more potent potassium binders, patiromer and sodium zirconium cyclosilicate.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
