{"title":"心肌梗死后细胞治疗的免疫调节作用。","authors":"Joseph B Moore, Marcin Wysoczynski","doi":"10.33696/immunology.3.082","DOIUrl":null,"url":null,"abstract":"Myocardial infarction (MI) due to coronary artery stenosis compromises vascular endothelial integrity and increases vascular permeability [1,2]. Concurrently, ensuing myocardial tissue death and necrosis results in the release of danger associated molecular patterns (DAMPs), cytokines, chemokines, bioactive lipids, as well as activation of the complement cascade [1-3]. Collectively, these events direct a pronounced and immediate immune response, which includes the recruitment of peripheral blood leukocytes to the site of injury [2,3]. These infiltrating neutrophils are primarily responsible for the clearance of necrotic tissue and cellular debris in ischemic regions via their release of a host of proteolytic enzymes/proteases. While this constitutes a necessary early step in the myocardial repair process at the site of injury, neutrophil-derived reactive oxygen species (ROS) and pro-inflammatory cytokines/chemokines can contribute to collateral damage of surviving myocardium and amplify tissue injury [3,4]. Nevertheless, neutrophils are imperative for proper infarct healing as their depletion prior to MI leads to a dysregulated immune response, excessive scarring, and impaired ventricular function [5]. Within days of an MI, neutrophils undergo cell death and disappear from infarcted tissue [3,4]. Recruitment of neutrophils is followed by two waves of monocyte infiltration. First, early recruitment of Ly6CHigh monocytes expressing pro-inflammatory cytokines, and second, infiltration of Ly6CLow monocytes with pro-resolving and pro-reparative function [3,6,7]. Ly6CHigh monocyte migration is driven by the presence of tissue CCL2 chemokine gradients and their interaction with their cognate receptor, CCR2 [8]—a group of monocytes that are principally sourced from bone marrow and spleen. Subsequently, these monocytes differentiate into Ly6CLowCCR2High macrophages, known as monocyte-derived macrophages [9,10]. These are distinct from Ly6CLowCCR2Low macrophages deposited in the myocardial tissue during embryonic development [11-13]. Both macrophage populations (Ly6CLowCCR2High and Ly6CLowCCR2Low) contribute to myocardial repair by clearance of dead tissue via efferocytosis and production of pro-reparative and pro-resolving mediators. Macrophagederived cytokines play an essential role in the proliferation and activation of cardiac fibroblasts (fibroblast-myofibroblast conversion) that deposit collagen at the site of injury. This process of scar formation fulfills the immediate need to preserve the structural integrity","PeriodicalId":73644,"journal":{"name":"Journal of cellular immunology","volume":"3 2","pages":"85-90"},"PeriodicalIF":0.0000,"publicationDate":"2021-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8098722/pdf/","citationCount":"3","resultStr":"{\"title\":\"Immunomodulatory Effects of Cell Therapy after Myocardial Infarction.\",\"authors\":\"Joseph B Moore, Marcin Wysoczynski\",\"doi\":\"10.33696/immunology.3.082\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Myocardial infarction (MI) due to coronary artery stenosis compromises vascular endothelial integrity and increases vascular permeability [1,2]. Concurrently, ensuing myocardial tissue death and necrosis results in the release of danger associated molecular patterns (DAMPs), cytokines, chemokines, bioactive lipids, as well as activation of the complement cascade [1-3]. Collectively, these events direct a pronounced and immediate immune response, which includes the recruitment of peripheral blood leukocytes to the site of injury [2,3]. These infiltrating neutrophils are primarily responsible for the clearance of necrotic tissue and cellular debris in ischemic regions via their release of a host of proteolytic enzymes/proteases. While this constitutes a necessary early step in the myocardial repair process at the site of injury, neutrophil-derived reactive oxygen species (ROS) and pro-inflammatory cytokines/chemokines can contribute to collateral damage of surviving myocardium and amplify tissue injury [3,4]. Nevertheless, neutrophils are imperative for proper infarct healing as their depletion prior to MI leads to a dysregulated immune response, excessive scarring, and impaired ventricular function [5]. Within days of an MI, neutrophils undergo cell death and disappear from infarcted tissue [3,4]. Recruitment of neutrophils is followed by two waves of monocyte infiltration. First, early recruitment of Ly6CHigh monocytes expressing pro-inflammatory cytokines, and second, infiltration of Ly6CLow monocytes with pro-resolving and pro-reparative function [3,6,7]. Ly6CHigh monocyte migration is driven by the presence of tissue CCL2 chemokine gradients and their interaction with their cognate receptor, CCR2 [8]—a group of monocytes that are principally sourced from bone marrow and spleen. Subsequently, these monocytes differentiate into Ly6CLowCCR2High macrophages, known as monocyte-derived macrophages [9,10]. These are distinct from Ly6CLowCCR2Low macrophages deposited in the myocardial tissue during embryonic development [11-13]. Both macrophage populations (Ly6CLowCCR2High and Ly6CLowCCR2Low) contribute to myocardial repair by clearance of dead tissue via efferocytosis and production of pro-reparative and pro-resolving mediators. Macrophagederived cytokines play an essential role in the proliferation and activation of cardiac fibroblasts (fibroblast-myofibroblast conversion) that deposit collagen at the site of injury. This process of scar formation fulfills the immediate need to preserve the structural integrity\",\"PeriodicalId\":73644,\"journal\":{\"name\":\"Journal of cellular immunology\",\"volume\":\"3 2\",\"pages\":\"85-90\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8098722/pdf/\",\"citationCount\":\"3\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of cellular immunology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.33696/immunology.3.082\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of cellular immunology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.33696/immunology.3.082","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Immunomodulatory Effects of Cell Therapy after Myocardial Infarction.
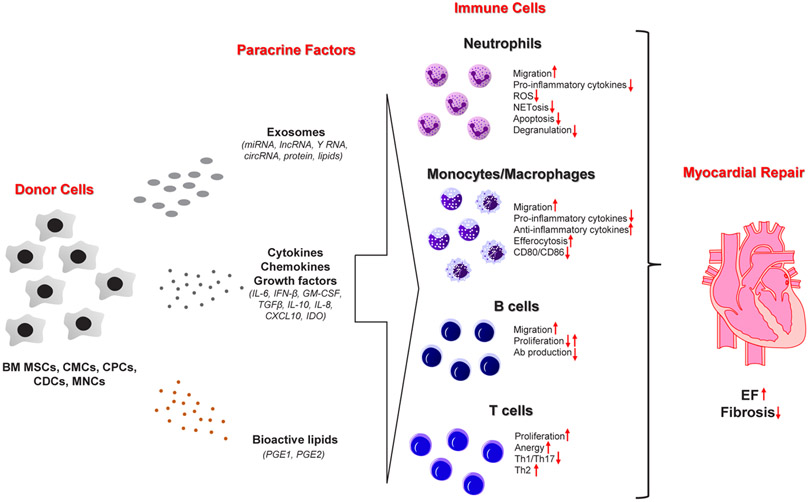
Myocardial infarction (MI) due to coronary artery stenosis compromises vascular endothelial integrity and increases vascular permeability [1,2]. Concurrently, ensuing myocardial tissue death and necrosis results in the release of danger associated molecular patterns (DAMPs), cytokines, chemokines, bioactive lipids, as well as activation of the complement cascade [1-3]. Collectively, these events direct a pronounced and immediate immune response, which includes the recruitment of peripheral blood leukocytes to the site of injury [2,3]. These infiltrating neutrophils are primarily responsible for the clearance of necrotic tissue and cellular debris in ischemic regions via their release of a host of proteolytic enzymes/proteases. While this constitutes a necessary early step in the myocardial repair process at the site of injury, neutrophil-derived reactive oxygen species (ROS) and pro-inflammatory cytokines/chemokines can contribute to collateral damage of surviving myocardium and amplify tissue injury [3,4]. Nevertheless, neutrophils are imperative for proper infarct healing as their depletion prior to MI leads to a dysregulated immune response, excessive scarring, and impaired ventricular function [5]. Within days of an MI, neutrophils undergo cell death and disappear from infarcted tissue [3,4]. Recruitment of neutrophils is followed by two waves of monocyte infiltration. First, early recruitment of Ly6CHigh monocytes expressing pro-inflammatory cytokines, and second, infiltration of Ly6CLow monocytes with pro-resolving and pro-reparative function [3,6,7]. Ly6CHigh monocyte migration is driven by the presence of tissue CCL2 chemokine gradients and their interaction with their cognate receptor, CCR2 [8]—a group of monocytes that are principally sourced from bone marrow and spleen. Subsequently, these monocytes differentiate into Ly6CLowCCR2High macrophages, known as monocyte-derived macrophages [9,10]. These are distinct from Ly6CLowCCR2Low macrophages deposited in the myocardial tissue during embryonic development [11-13]. Both macrophage populations (Ly6CLowCCR2High and Ly6CLowCCR2Low) contribute to myocardial repair by clearance of dead tissue via efferocytosis and production of pro-reparative and pro-resolving mediators. Macrophagederived cytokines play an essential role in the proliferation and activation of cardiac fibroblasts (fibroblast-myofibroblast conversion) that deposit collagen at the site of injury. This process of scar formation fulfills the immediate need to preserve the structural integrity



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
