Juan D Salcedo Betancourt, Oscar A Garcia Valencia, Victor G Becerra-Gonzales, Karla G Carias Martinez, Jennifer Chapman, Natalia Yanchenko, Marco A Ladino
{"title":"双侧肾伯基特淋巴瘤患者的严重b型乳酸酸中毒。","authors":"Juan D Salcedo Betancourt, Oscar A Garcia Valencia, Victor G Becerra-Gonzales, Karla G Carias Martinez, Jennifer Chapman, Natalia Yanchenko, Marco A Ladino","doi":"10.5414/CNCS110123","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Lactic acidosis (LA) can be categorized as type A, which occurs in the presence of tissue hypoxia, or type B, occurring in the absence of tissue hypoxia. Hematologic malignancies are an uncommon cause of type B LA.</p><p><strong>Case presentation: </strong>A 63-year-old man, HIV-negative, with a history of diabetes mellitus, hypothyroidism, and non-alcoholic fatty liver disease (NAFLD), presented to the ED complaining of acute-on-chronic lumbar pain, and was found to have high serum anion gap (AG) LA. The rest of chemistry and infectious workup was within normal limits. Despite bicarbonate therapy and fluid resuscitation, the patient remained with persistent AG metabolic acidosis and increasing lactic acid up to 14.5 mmol/L. An abdominal computerized tomography (CT) revealed multiple bilateral enhancing lesions in the kidneys, as well as gastric wall thickening. Upper gastrointestinal endoscopy with biopsy showed a high-grade Burkitt's lymphoma. Further staging showed bone marrow involvement and extensive abdominal adenopathy. After two cycles of inpatient chemotherapy with dose-adjusted EPOCH-R (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin and rituximab), the patient developed multifocal pneumonia complicated by respiratory failure. Following a prolonged ICU stay, after discussion with the family members, a decision of withdrawal of life-sustaining therapy was reached.</p><p><strong>Conclusion: </strong>Persistent LA, without identifiable causes of tissue hypoxia, should prompt clinicians to suspect non-hypoxic etiologies, including occult high-grade malignancies. Hematological malignancies constitute an extremely rare cause of type-B LA, carrying a poor prognosis.</p>","PeriodicalId":10398,"journal":{"name":"Clinical Nephrology. Case Studies","volume":"9 ","pages":"49-53"},"PeriodicalIF":0.0000,"publicationDate":"2021-04-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8079968/pdf/","citationCount":"1","resultStr":"{\"title\":\"Severe type-B lactic acidosis in a patient with bilateral renal Burkitt's lymphoma.\",\"authors\":\"Juan D Salcedo Betancourt, Oscar A Garcia Valencia, Victor G Becerra-Gonzales, Karla G Carias Martinez, Jennifer Chapman, Natalia Yanchenko, Marco A Ladino\",\"doi\":\"10.5414/CNCS110123\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Lactic acidosis (LA) can be categorized as type A, which occurs in the presence of tissue hypoxia, or type B, occurring in the absence of tissue hypoxia. Hematologic malignancies are an uncommon cause of type B LA.</p><p><strong>Case presentation: </strong>A 63-year-old man, HIV-negative, with a history of diabetes mellitus, hypothyroidism, and non-alcoholic fatty liver disease (NAFLD), presented to the ED complaining of acute-on-chronic lumbar pain, and was found to have high serum anion gap (AG) LA. The rest of chemistry and infectious workup was within normal limits. Despite bicarbonate therapy and fluid resuscitation, the patient remained with persistent AG metabolic acidosis and increasing lactic acid up to 14.5 mmol/L. An abdominal computerized tomography (CT) revealed multiple bilateral enhancing lesions in the kidneys, as well as gastric wall thickening. Upper gastrointestinal endoscopy with biopsy showed a high-grade Burkitt's lymphoma. Further staging showed bone marrow involvement and extensive abdominal adenopathy. After two cycles of inpatient chemotherapy with dose-adjusted EPOCH-R (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin and rituximab), the patient developed multifocal pneumonia complicated by respiratory failure. Following a prolonged ICU stay, after discussion with the family members, a decision of withdrawal of life-sustaining therapy was reached.</p><p><strong>Conclusion: </strong>Persistent LA, without identifiable causes of tissue hypoxia, should prompt clinicians to suspect non-hypoxic etiologies, including occult high-grade malignancies. Hematological malignancies constitute an extremely rare cause of type-B LA, carrying a poor prognosis.</p>\",\"PeriodicalId\":10398,\"journal\":{\"name\":\"Clinical Nephrology. Case Studies\",\"volume\":\"9 \",\"pages\":\"49-53\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-04-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8079968/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Nephrology. Case Studies\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5414/CNCS110123\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nephrology. Case Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS110123","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Severe type-B lactic acidosis in a patient with bilateral renal Burkitt's lymphoma.
Introduction: Lactic acidosis (LA) can be categorized as type A, which occurs in the presence of tissue hypoxia, or type B, occurring in the absence of tissue hypoxia. Hematologic malignancies are an uncommon cause of type B LA.
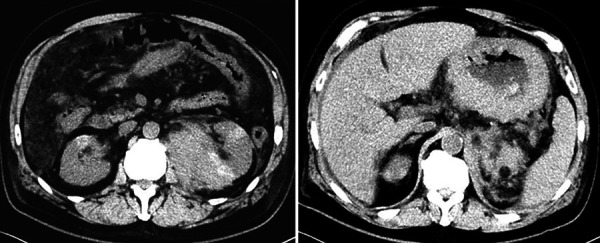
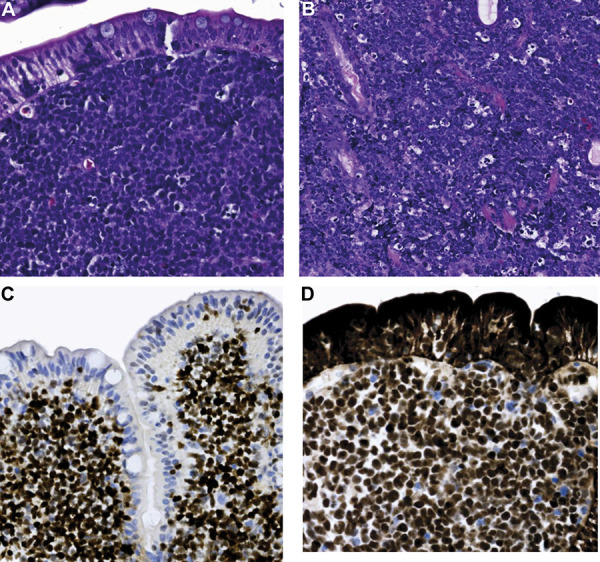
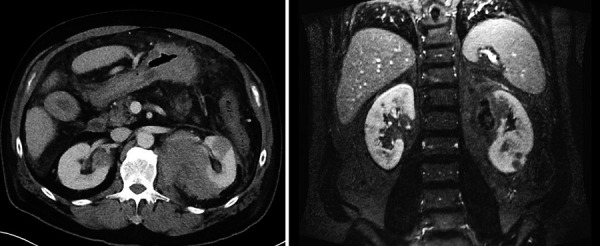
Case presentation: A 63-year-old man, HIV-negative, with a history of diabetes mellitus, hypothyroidism, and non-alcoholic fatty liver disease (NAFLD), presented to the ED complaining of acute-on-chronic lumbar pain, and was found to have high serum anion gap (AG) LA. The rest of chemistry and infectious workup was within normal limits. Despite bicarbonate therapy and fluid resuscitation, the patient remained with persistent AG metabolic acidosis and increasing lactic acid up to 14.5 mmol/L. An abdominal computerized tomography (CT) revealed multiple bilateral enhancing lesions in the kidneys, as well as gastric wall thickening. Upper gastrointestinal endoscopy with biopsy showed a high-grade Burkitt's lymphoma. Further staging showed bone marrow involvement and extensive abdominal adenopathy. After two cycles of inpatient chemotherapy with dose-adjusted EPOCH-R (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin and rituximab), the patient developed multifocal pneumonia complicated by respiratory failure. Following a prolonged ICU stay, after discussion with the family members, a decision of withdrawal of life-sustaining therapy was reached.
Conclusion: Persistent LA, without identifiable causes of tissue hypoxia, should prompt clinicians to suspect non-hypoxic etiologies, including occult high-grade malignancies. Hematological malignancies constitute an extremely rare cause of type-B LA, carrying a poor prognosis.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
