Sebastian Holm, Olof Engström, Ida Petäjä, Fredrik Huss
{"title":"入院时对烧伤程度的估计与出院时的评估是否不同?","authors":"Sebastian Holm, Olof Engström, Ida Petäjä, Fredrik Huss","doi":"10.1177/20595131211019403","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Estimation of total body surface area (TBSA) burnt and burn depth are among the most central parts of acute burn assessment/treatment as they determine the level and type of care needed. Traditional methods for determining burn extent on admission often lead to inaccurate estimations, especially in paediatric or overweight patients.</p><p><strong>Aim: </strong>To compare %TBSA at admission with validated %TBSA at discharge in different patient populations to investigate if significant over- or underestimation occurs.</p><p><strong>Method: </strong>This retrospective observational study is based on a patient registry of all the patients (n = 863) treated at the Uppsala University Hospital's Burn Centre between 2010 and 2018. The patients were divided into subgroups based on age, gender, body mass index (BMI) and validated burn extent. The %TBSA estimated at admission was compared to the validated %TBSA in all groups separately.</p><p><strong>Results: </strong>As has been published before, we also found that the %TBSA in paediatric patients was more often overestimated as were the smaller injuries, whereas larger injuries were often underestimated. BMI did not clearly affect the estimations and there was no clear difference between the genders in estimated %TBSA.</p><p><strong>Conclusion: </strong>Inaccurate estimations of %TBSA are common, particularly for paediatric patients and small or large injuries. We recommend a careful accurate approach when calculating %TBSA in the paediatric population to avoid over- and under-resuscitation. Increased education and training are recommended to improve accurate estimation in the future.</p><p><strong>Lay summary: </strong>The correct estimation of both extent and depth of burn is very important. This assessment guides the lever of care needed, the necessary amount of fluid resuscitation, the predicted outcome and more. It has been proven notably difficult to correct assess, especially the extent of a burn. Despite different tools as the \"Rule of Nine\" (body area divided into multiples of 9% body surfaces), the \"Rule of Palm\" (Patient's palm, fingers included, approximates 1% of body surfaces), the Lund & Browder chart (detailed, age-specific body areas) and different more technical solutions. Often inaccurate estimations are done which thus affect the treatment. This depth and extent estimation is usually performed when the patient is admitted. However, it is known that burns change appearance during the first few days of care. In our Burn Center we have also performed this estimation when the patient is discharged. At this point it is known the true extent and depth of the initial burn. In this retrospective observational study, we compared the burn extent estimated on admission with the one on discharge to investigate whether the initial assessment is accurate. This study highlights the issue of frequent inaccurate burn extent estimations, especially in subgroups as overweight patient or pediatric patients.</p>","PeriodicalId":21495,"journal":{"name":"Scars, burns & healing","volume":"7 ","pages":"20595131211019403"},"PeriodicalIF":0.0000,"publicationDate":"2021-06-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bb/72/10.1177_20595131211019403.PMC8221698.pdf","citationCount":"0","resultStr":"{\"title\":\"Does the estimation of burn extent at admission differ from the assessment at discharge?\",\"authors\":\"Sebastian Holm, Olof Engström, Ida Petäjä, Fredrik Huss\",\"doi\":\"10.1177/20595131211019403\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Estimation of total body surface area (TBSA) burnt and burn depth are among the most central parts of acute burn assessment/treatment as they determine the level and type of care needed. Traditional methods for determining burn extent on admission often lead to inaccurate estimations, especially in paediatric or overweight patients.</p><p><strong>Aim: </strong>To compare %TBSA at admission with validated %TBSA at discharge in different patient populations to investigate if significant over- or underestimation occurs.</p><p><strong>Method: </strong>This retrospective observational study is based on a patient registry of all the patients (n = 863) treated at the Uppsala University Hospital's Burn Centre between 2010 and 2018. The patients were divided into subgroups based on age, gender, body mass index (BMI) and validated burn extent. The %TBSA estimated at admission was compared to the validated %TBSA in all groups separately.</p><p><strong>Results: </strong>As has been published before, we also found that the %TBSA in paediatric patients was more often overestimated as were the smaller injuries, whereas larger injuries were often underestimated. BMI did not clearly affect the estimations and there was no clear difference between the genders in estimated %TBSA.</p><p><strong>Conclusion: </strong>Inaccurate estimations of %TBSA are common, particularly for paediatric patients and small or large injuries. We recommend a careful accurate approach when calculating %TBSA in the paediatric population to avoid over- and under-resuscitation. Increased education and training are recommended to improve accurate estimation in the future.</p><p><strong>Lay summary: </strong>The correct estimation of both extent and depth of burn is very important. This assessment guides the lever of care needed, the necessary amount of fluid resuscitation, the predicted outcome and more. It has been proven notably difficult to correct assess, especially the extent of a burn. Despite different tools as the \\\"Rule of Nine\\\" (body area divided into multiples of 9% body surfaces), the \\\"Rule of Palm\\\" (Patient's palm, fingers included, approximates 1% of body surfaces), the Lund & Browder chart (detailed, age-specific body areas) and different more technical solutions. Often inaccurate estimations are done which thus affect the treatment. This depth and extent estimation is usually performed when the patient is admitted. However, it is known that burns change appearance during the first few days of care. In our Burn Center we have also performed this estimation when the patient is discharged. At this point it is known the true extent and depth of the initial burn. In this retrospective observational study, we compared the burn extent estimated on admission with the one on discharge to investigate whether the initial assessment is accurate. This study highlights the issue of frequent inaccurate burn extent estimations, especially in subgroups as overweight patient or pediatric patients.</p>\",\"PeriodicalId\":21495,\"journal\":{\"name\":\"Scars, burns & healing\",\"volume\":\"7 \",\"pages\":\"20595131211019403\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-06-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bb/72/10.1177_20595131211019403.PMC8221698.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Scars, burns & healing\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20595131211019403\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scars, burns & healing","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20595131211019403","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Does the estimation of burn extent at admission differ from the assessment at discharge?
Introduction: Estimation of total body surface area (TBSA) burnt and burn depth are among the most central parts of acute burn assessment/treatment as they determine the level and type of care needed. Traditional methods for determining burn extent on admission often lead to inaccurate estimations, especially in paediatric or overweight patients.
Aim: To compare %TBSA at admission with validated %TBSA at discharge in different patient populations to investigate if significant over- or underestimation occurs.
Method: This retrospective observational study is based on a patient registry of all the patients (n = 863) treated at the Uppsala University Hospital's Burn Centre between 2010 and 2018. The patients were divided into subgroups based on age, gender, body mass index (BMI) and validated burn extent. The %TBSA estimated at admission was compared to the validated %TBSA in all groups separately.
Results: As has been published before, we also found that the %TBSA in paediatric patients was more often overestimated as were the smaller injuries, whereas larger injuries were often underestimated. BMI did not clearly affect the estimations and there was no clear difference between the genders in estimated %TBSA.
Conclusion: Inaccurate estimations of %TBSA are common, particularly for paediatric patients and small or large injuries. We recommend a careful accurate approach when calculating %TBSA in the paediatric population to avoid over- and under-resuscitation. Increased education and training are recommended to improve accurate estimation in the future.
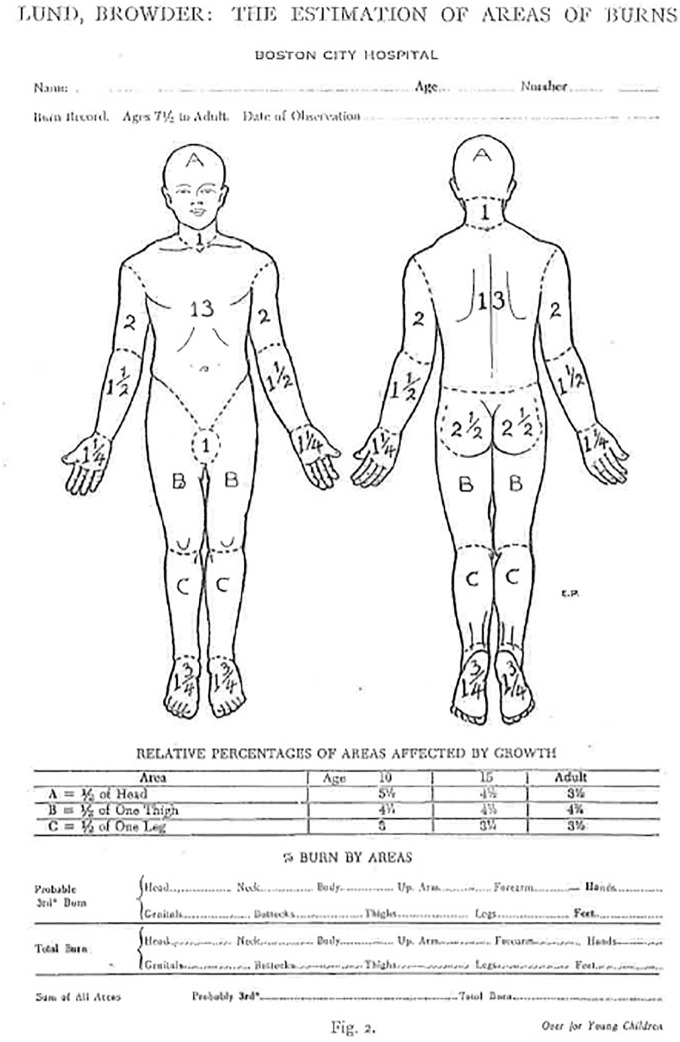
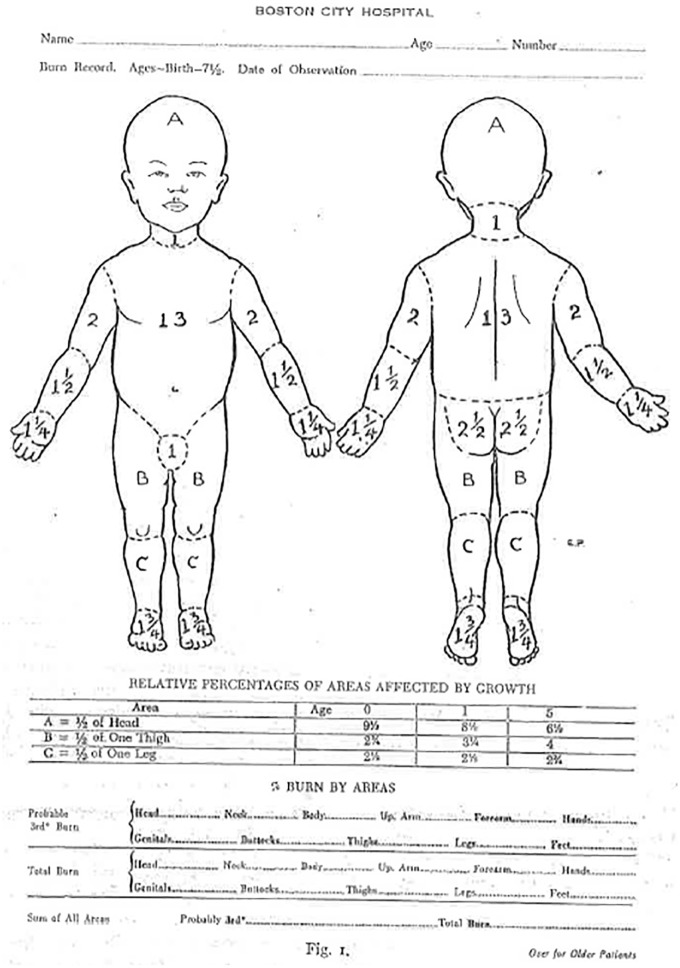
Lay summary: The correct estimation of both extent and depth of burn is very important. This assessment guides the lever of care needed, the necessary amount of fluid resuscitation, the predicted outcome and more. It has been proven notably difficult to correct assess, especially the extent of a burn. Despite different tools as the "Rule of Nine" (body area divided into multiples of 9% body surfaces), the "Rule of Palm" (Patient's palm, fingers included, approximates 1% of body surfaces), the Lund & Browder chart (detailed, age-specific body areas) and different more technical solutions. Often inaccurate estimations are done which thus affect the treatment. This depth and extent estimation is usually performed when the patient is admitted. However, it is known that burns change appearance during the first few days of care. In our Burn Center we have also performed this estimation when the patient is discharged. At this point it is known the true extent and depth of the initial burn. In this retrospective observational study, we compared the burn extent estimated on admission with the one on discharge to investigate whether the initial assessment is accurate. This study highlights the issue of frequent inaccurate burn extent estimations, especially in subgroups as overweight patient or pediatric patients.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
