Luke L Wang, Brandon L Henslee, Peter B Sam, Chad A LaGrange, Shawna L Boyle
{"title":"Biopsy-Naïve患者获得mri融合活检的最佳PSA阈值。","authors":"Luke L Wang, Brandon L Henslee, Peter B Sam, Chad A LaGrange, Shawna L Boyle","doi":"10.1155/2021/5531511","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>The study investigates the prostate-specific antigen threshold for adding targeted, software-based, magnetic resonance imaging-ultrasound fusion biopsy during a standard 12-core biopsy in biopsy-naïve patients. It secondarily explores whether the targeted biopsy is necessary in setting of abnormal digital rectal examination.</p><p><strong>Methods: </strong>260 patients with suspected localized prostate cancer with no prior biopsy underwent prostate magnetic resonance imaging and were found to have Prostate Imaging Reporting and Data System score ≥ 3 lesion(s). All 260 patients underwent standard 12-core biopsy and targeted biopsy during the same session. Clinically significant cancer was Gleason ≥3 + 4.</p><p><strong>Results: </strong>Percentages of patients with prostate-specific antigen 0-1.99, 2-3.99, 4-4.99, 5-5.99, 6-9.99, and ≥10 were 3.0%, 4.7%, 20.8%, 16.9%, 37.7%, and 16.9%, respectively. Cumulative frequency of clinically significant prostate cancer increased with the addition of targeted biopsy compared with standard biopsy alone across all prostate-specific antigen ranges. The difference in clinically significant cancer detection between targeted plus standard biopsy compared to standard biopsy alone becomes statistically significant at prostate-specific antigen >4.3 (<i>p</i>=0.031). At this threshold, combination biopsy detected 20 clinically significant prostate cancers, while standard detected 14 with 88% sensitivity and 20% specificity. Excluding targeted biopsy in setting of a positive digital rectal exam would save 12.3% magnetic resonance imaging and miss 1.8% clinically significant cancers in our cohort.</p><p><strong>Conclusions: </strong>In biopsy-naïve patients, at prostate-specific antigen >4.3, there is a significant increase in clinically significant prostate cancer detection when targeted biopsy is added to standard biopsy. Obtaining standard biopsy alone in patients with abnormal digital rectal examinations would miss 1.8% clinically significant cancers in our cohort.</p>","PeriodicalId":20907,"journal":{"name":"Prostate Cancer","volume":"2021 ","pages":"5531511"},"PeriodicalIF":2.0000,"publicationDate":"2021-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8266472/pdf/","citationCount":"0","resultStr":"{\"title\":\"Optimal PSA Threshold for Obtaining MRI-Fusion Biopsy in Biopsy-Naïve Patients.\",\"authors\":\"Luke L Wang, Brandon L Henslee, Peter B Sam, Chad A LaGrange, Shawna L Boyle\",\"doi\":\"10.1155/2021/5531511\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>The study investigates the prostate-specific antigen threshold for adding targeted, software-based, magnetic resonance imaging-ultrasound fusion biopsy during a standard 12-core biopsy in biopsy-naïve patients. It secondarily explores whether the targeted biopsy is necessary in setting of abnormal digital rectal examination.</p><p><strong>Methods: </strong>260 patients with suspected localized prostate cancer with no prior biopsy underwent prostate magnetic resonance imaging and were found to have Prostate Imaging Reporting and Data System score ≥ 3 lesion(s). All 260 patients underwent standard 12-core biopsy and targeted biopsy during the same session. Clinically significant cancer was Gleason ≥3 + 4.</p><p><strong>Results: </strong>Percentages of patients with prostate-specific antigen 0-1.99, 2-3.99, 4-4.99, 5-5.99, 6-9.99, and ≥10 were 3.0%, 4.7%, 20.8%, 16.9%, 37.7%, and 16.9%, respectively. Cumulative frequency of clinically significant prostate cancer increased with the addition of targeted biopsy compared with standard biopsy alone across all prostate-specific antigen ranges. The difference in clinically significant cancer detection between targeted plus standard biopsy compared to standard biopsy alone becomes statistically significant at prostate-specific antigen >4.3 (<i>p</i>=0.031). At this threshold, combination biopsy detected 20 clinically significant prostate cancers, while standard detected 14 with 88% sensitivity and 20% specificity. Excluding targeted biopsy in setting of a positive digital rectal exam would save 12.3% magnetic resonance imaging and miss 1.8% clinically significant cancers in our cohort.</p><p><strong>Conclusions: </strong>In biopsy-naïve patients, at prostate-specific antigen >4.3, there is a significant increase in clinically significant prostate cancer detection when targeted biopsy is added to standard biopsy. Obtaining standard biopsy alone in patients with abnormal digital rectal examinations would miss 1.8% clinically significant cancers in our cohort.</p>\",\"PeriodicalId\":20907,\"journal\":{\"name\":\"Prostate Cancer\",\"volume\":\"2021 \",\"pages\":\"5531511\"},\"PeriodicalIF\":2.0000,\"publicationDate\":\"2021-07-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8266472/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Prostate Cancer\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2021/5531511\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Prostate Cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/5531511","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Optimal PSA Threshold for Obtaining MRI-Fusion Biopsy in Biopsy-Naïve Patients.
Objective: The study investigates the prostate-specific antigen threshold for adding targeted, software-based, magnetic resonance imaging-ultrasound fusion biopsy during a standard 12-core biopsy in biopsy-naïve patients. It secondarily explores whether the targeted biopsy is necessary in setting of abnormal digital rectal examination.
Methods: 260 patients with suspected localized prostate cancer with no prior biopsy underwent prostate magnetic resonance imaging and were found to have Prostate Imaging Reporting and Data System score ≥ 3 lesion(s). All 260 patients underwent standard 12-core biopsy and targeted biopsy during the same session. Clinically significant cancer was Gleason ≥3 + 4.
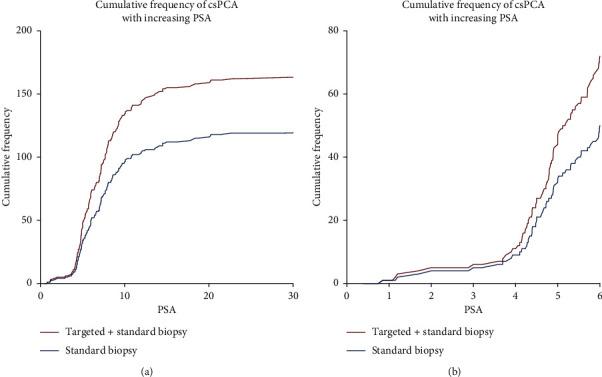
Results: Percentages of patients with prostate-specific antigen 0-1.99, 2-3.99, 4-4.99, 5-5.99, 6-9.99, and ≥10 were 3.0%, 4.7%, 20.8%, 16.9%, 37.7%, and 16.9%, respectively. Cumulative frequency of clinically significant prostate cancer increased with the addition of targeted biopsy compared with standard biopsy alone across all prostate-specific antigen ranges. The difference in clinically significant cancer detection between targeted plus standard biopsy compared to standard biopsy alone becomes statistically significant at prostate-specific antigen >4.3 (p=0.031). At this threshold, combination biopsy detected 20 clinically significant prostate cancers, while standard detected 14 with 88% sensitivity and 20% specificity. Excluding targeted biopsy in setting of a positive digital rectal exam would save 12.3% magnetic resonance imaging and miss 1.8% clinically significant cancers in our cohort.
Conclusions: In biopsy-naïve patients, at prostate-specific antigen >4.3, there is a significant increase in clinically significant prostate cancer detection when targeted biopsy is added to standard biopsy. Obtaining standard biopsy alone in patients with abnormal digital rectal examinations would miss 1.8% clinically significant cancers in our cohort.
期刊介绍:
Prostate Cancer is a peer-reviewed, Open Access journal that provides a multidisciplinary platform for scientists, surgeons, oncologists and clinicians working on prostate cancer. The journal publishes original research articles, review articles, and clinical studies related to the diagnosis, surgery, radiotherapy, drug discovery and medical management of the disease.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
