Friederike Austein, Antonia Carlotta Fischer, Jens Fiehler, Olav Jansen, Thomas Lindner, Susanne Gellißen
{"title":"灌注CT对血管内治疗后脑出血的预测价值。","authors":"Friederike Austein, Antonia Carlotta Fischer, Jens Fiehler, Olav Jansen, Thomas Lindner, Susanne Gellißen","doi":"10.1155/2021/9933015","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Intracerebral hemorrhage (ICH) is a serious complication of endovascular treatment (EVT) in stroke patients with large vessel occlusion (LVO) and associated with increased morbidity and mortality.</p><p><strong>Aims: </strong>Identification of radiological predictors is highly relevant. We investigated the predictive power of computed tomography perfusion (CTP) parameters concerning ICH in patients receiving EVT.</p><p><strong>Methods: </strong>392 patients with anterior circulation LVO with multimodal CT imaging who underwent EVT were analyzed. CTP parameters were visually evaluated for modified ASPECTS regions and compared between patients without ICH, those with hemorrhagic infarction (HI), and those with parenchymal hematoma (PH) according to the ECASS criteria at follow-up imaging and broken down by ASPECTS regions.</p><p><strong>Results: </strong>168 received intravenous thrombolysis (IV-rtPA), and 115 developed subsequent ICH (29.3%), of which 74 were classified as HI and 41 as PH. Patients with HI and PH had lower ASPECTS than patients without ICH and worse functional outcome after 90 days (<i>p</i> < 0.05). In 102 of the 115 patients with ICH, the deep middle cerebral artery (MCA) territory was affected with differences between patients without ICH, those with HI, and those with PH regarding cerebral blood volume (CBV) and blood-brain barrier permeability measured as flow extraction product (FED) relative to the contralateral hemisphere (<i>p</i> < 0.05). Patients with PH showed larger perfusion CT infarct core than patients without ICH (<i>p</i> < 0.01).</p><p><strong>Conclusion: </strong>None of the examined CTP parameters was found to be a strong predictor of subsequent ICH. ASPECTS and initial CTP core volume were more reliable and may be useful and even so more practicable to assess the risk of subsequent ICH after EVT.</p>","PeriodicalId":22054,"journal":{"name":"Stroke Research and Treatment","volume":null,"pages":null},"PeriodicalIF":1.8000,"publicationDate":"2021-07-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8321751/pdf/","citationCount":"6","resultStr":"{\"title\":\"Value of Perfusion CT in the Prediction of Intracerebral Hemorrhage after Endovascular Treatment.\",\"authors\":\"Friederike Austein, Antonia Carlotta Fischer, Jens Fiehler, Olav Jansen, Thomas Lindner, Susanne Gellißen\",\"doi\":\"10.1155/2021/9933015\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Intracerebral hemorrhage (ICH) is a serious complication of endovascular treatment (EVT) in stroke patients with large vessel occlusion (LVO) and associated with increased morbidity and mortality.</p><p><strong>Aims: </strong>Identification of radiological predictors is highly relevant. We investigated the predictive power of computed tomography perfusion (CTP) parameters concerning ICH in patients receiving EVT.</p><p><strong>Methods: </strong>392 patients with anterior circulation LVO with multimodal CT imaging who underwent EVT were analyzed. CTP parameters were visually evaluated for modified ASPECTS regions and compared between patients without ICH, those with hemorrhagic infarction (HI), and those with parenchymal hematoma (PH) according to the ECASS criteria at follow-up imaging and broken down by ASPECTS regions.</p><p><strong>Results: </strong>168 received intravenous thrombolysis (IV-rtPA), and 115 developed subsequent ICH (29.3%), of which 74 were classified as HI and 41 as PH. Patients with HI and PH had lower ASPECTS than patients without ICH and worse functional outcome after 90 days (<i>p</i> < 0.05). In 102 of the 115 patients with ICH, the deep middle cerebral artery (MCA) territory was affected with differences between patients without ICH, those with HI, and those with PH regarding cerebral blood volume (CBV) and blood-brain barrier permeability measured as flow extraction product (FED) relative to the contralateral hemisphere (<i>p</i> < 0.05). Patients with PH showed larger perfusion CT infarct core than patients without ICH (<i>p</i> < 0.01).</p><p><strong>Conclusion: </strong>None of the examined CTP parameters was found to be a strong predictor of subsequent ICH. ASPECTS and initial CTP core volume were more reliable and may be useful and even so more practicable to assess the risk of subsequent ICH after EVT.</p>\",\"PeriodicalId\":22054,\"journal\":{\"name\":\"Stroke Research and Treatment\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2021-07-22\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8321751/pdf/\",\"citationCount\":\"6\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Stroke Research and Treatment\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2021/9933015\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stroke Research and Treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/9933015","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
Value of Perfusion CT in the Prediction of Intracerebral Hemorrhage after Endovascular Treatment.
Background: Intracerebral hemorrhage (ICH) is a serious complication of endovascular treatment (EVT) in stroke patients with large vessel occlusion (LVO) and associated with increased morbidity and mortality.
Aims: Identification of radiological predictors is highly relevant. We investigated the predictive power of computed tomography perfusion (CTP) parameters concerning ICH in patients receiving EVT.
Methods: 392 patients with anterior circulation LVO with multimodal CT imaging who underwent EVT were analyzed. CTP parameters were visually evaluated for modified ASPECTS regions and compared between patients without ICH, those with hemorrhagic infarction (HI), and those with parenchymal hematoma (PH) according to the ECASS criteria at follow-up imaging and broken down by ASPECTS regions.
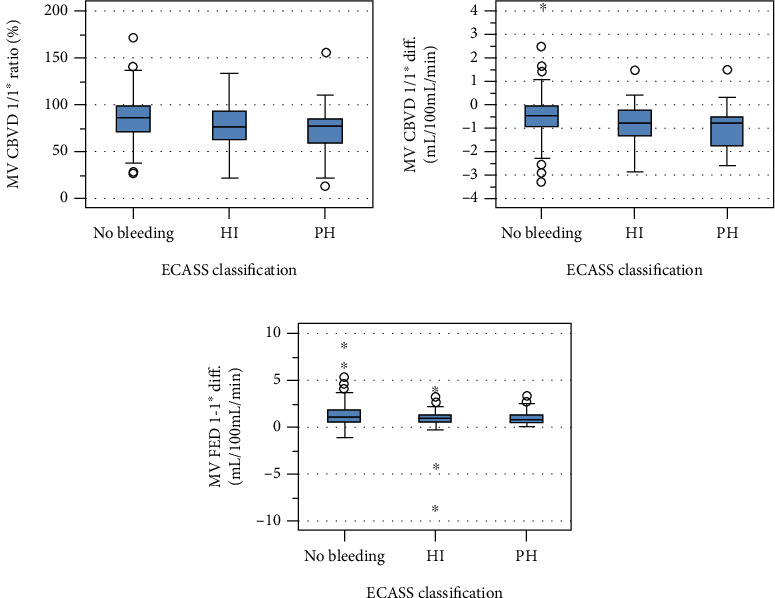
Results: 168 received intravenous thrombolysis (IV-rtPA), and 115 developed subsequent ICH (29.3%), of which 74 were classified as HI and 41 as PH. Patients with HI and PH had lower ASPECTS than patients without ICH and worse functional outcome after 90 days (p < 0.05). In 102 of the 115 patients with ICH, the deep middle cerebral artery (MCA) territory was affected with differences between patients without ICH, those with HI, and those with PH regarding cerebral blood volume (CBV) and blood-brain barrier permeability measured as flow extraction product (FED) relative to the contralateral hemisphere (p < 0.05). Patients with PH showed larger perfusion CT infarct core than patients without ICH (p < 0.01).
Conclusion: None of the examined CTP parameters was found to be a strong predictor of subsequent ICH. ASPECTS and initial CTP core volume were more reliable and may be useful and even so more practicable to assess the risk of subsequent ICH after EVT.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
