{"title":"髂腹下神经阻滞治疗持续性腰管综合征腹股沟疝患者腹股沟疼痛1例。","authors":"Takanori Sekito, Takuya Sadahira, Masahiro Sugihara, Kohei Edamura, Motoo Araki, Yasutomo Nasu","doi":"10.1155/2021/7577632","DOIUrl":null,"url":null,"abstract":"<p><p>Persistent Müllerian duct syndrome can cause an inguinal hernia, although this is a rare occurrence; recurrent inguinal hernias can, in turn, cause ongoing groin pain. Management of groin pain plays an important role in patients' quality of life. We present our experience with a 43-year-old man who had a 2-week history of left-sided groin pain. The patient underwent laparoscopic surgery for a left inguinal hernia via the transabdominal preperitoneal approach. Right-sided cryptorchidism was noted during surgery, with a solid structure-thought to be a uterus-extending into the left inguinal canal. The diagnosis was persistent Müllerian duct syndrome, and the groin pain was relieved after a laparoscopic right orchiectomy with a bilateral preperitoneal hernia repair using a mesh. Four years later, magnetic resonance imaging performed for new-onset left groin pain showed a left inguinal hernia caused by the uterine structure. We diagnosed the recurrent hernia as the cause of his pain. Prior to performing any invasive surgical procedures, an iliohypogastric nerve block was performed using 1% lidocaine. Short-term analgesia was provided by the block, improving his quality of life. He has been followed since then and has declined surgical neurectomy. An iliohypogastric nerve block can be an effective method of controlling groin pain caused by an inguinal hernia resulting from persistent Müllerian duct syndrome; the effectiveness of the nerve block will help determine whether surgical neurectomy is indicated for permanent pain control.</p>","PeriodicalId":30323,"journal":{"name":"Case Reports in Urology","volume":"2021 ","pages":"7577632"},"PeriodicalIF":0.0000,"publicationDate":"2021-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8376460/pdf/","citationCount":"0","resultStr":"{\"title\":\"Management of Groin Pain Using an Iliohypogastric Nerve Block in a Patient with Inguinal Hernia due to Persistent Müllerian Duct Syndrome.\",\"authors\":\"Takanori Sekito, Takuya Sadahira, Masahiro Sugihara, Kohei Edamura, Motoo Araki, Yasutomo Nasu\",\"doi\":\"10.1155/2021/7577632\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Persistent Müllerian duct syndrome can cause an inguinal hernia, although this is a rare occurrence; recurrent inguinal hernias can, in turn, cause ongoing groin pain. Management of groin pain plays an important role in patients' quality of life. We present our experience with a 43-year-old man who had a 2-week history of left-sided groin pain. The patient underwent laparoscopic surgery for a left inguinal hernia via the transabdominal preperitoneal approach. Right-sided cryptorchidism was noted during surgery, with a solid structure-thought to be a uterus-extending into the left inguinal canal. The diagnosis was persistent Müllerian duct syndrome, and the groin pain was relieved after a laparoscopic right orchiectomy with a bilateral preperitoneal hernia repair using a mesh. Four years later, magnetic resonance imaging performed for new-onset left groin pain showed a left inguinal hernia caused by the uterine structure. We diagnosed the recurrent hernia as the cause of his pain. Prior to performing any invasive surgical procedures, an iliohypogastric nerve block was performed using 1% lidocaine. Short-term analgesia was provided by the block, improving his quality of life. He has been followed since then and has declined surgical neurectomy. An iliohypogastric nerve block can be an effective method of controlling groin pain caused by an inguinal hernia resulting from persistent Müllerian duct syndrome; the effectiveness of the nerve block will help determine whether surgical neurectomy is indicated for permanent pain control.</p>\",\"PeriodicalId\":30323,\"journal\":{\"name\":\"Case Reports in Urology\",\"volume\":\"2021 \",\"pages\":\"7577632\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2021-08-12\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8376460/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Urology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2021/7577632\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/7577632","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Management of Groin Pain Using an Iliohypogastric Nerve Block in a Patient with Inguinal Hernia due to Persistent Müllerian Duct Syndrome.
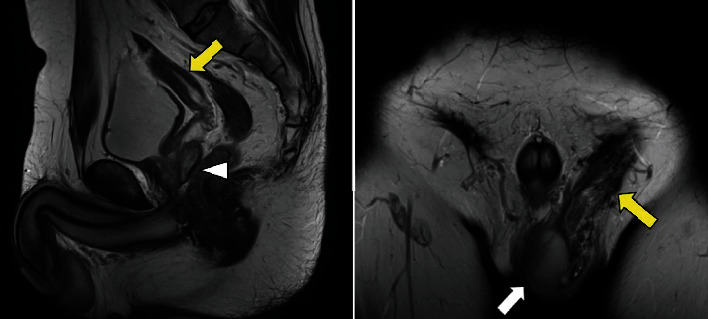
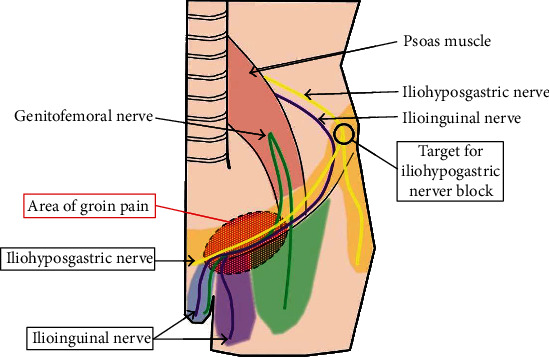
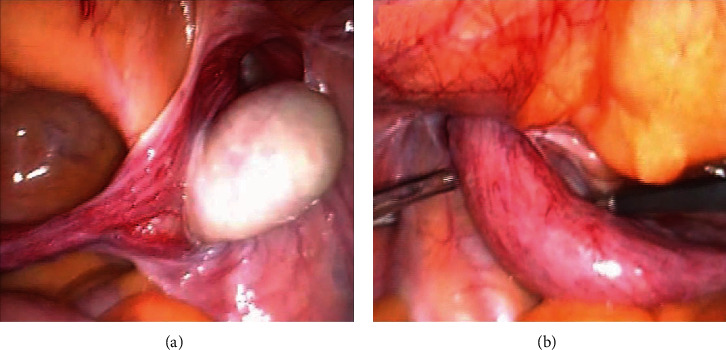
Persistent Müllerian duct syndrome can cause an inguinal hernia, although this is a rare occurrence; recurrent inguinal hernias can, in turn, cause ongoing groin pain. Management of groin pain plays an important role in patients' quality of life. We present our experience with a 43-year-old man who had a 2-week history of left-sided groin pain. The patient underwent laparoscopic surgery for a left inguinal hernia via the transabdominal preperitoneal approach. Right-sided cryptorchidism was noted during surgery, with a solid structure-thought to be a uterus-extending into the left inguinal canal. The diagnosis was persistent Müllerian duct syndrome, and the groin pain was relieved after a laparoscopic right orchiectomy with a bilateral preperitoneal hernia repair using a mesh. Four years later, magnetic resonance imaging performed for new-onset left groin pain showed a left inguinal hernia caused by the uterine structure. We diagnosed the recurrent hernia as the cause of his pain. Prior to performing any invasive surgical procedures, an iliohypogastric nerve block was performed using 1% lidocaine. Short-term analgesia was provided by the block, improving his quality of life. He has been followed since then and has declined surgical neurectomy. An iliohypogastric nerve block can be an effective method of controlling groin pain caused by an inguinal hernia resulting from persistent Müllerian duct syndrome; the effectiveness of the nerve block will help determine whether surgical neurectomy is indicated for permanent pain control.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
