Jin Cho, Krystal Place, Rebecca Salstrand, Monireh Rahmat, Misagh Mansouri, Nancy Fell, Mina Sartipi
{"title":"开发中风后患者出院处置预测工具,并进行 30 天再入院验证。","authors":"Jin Cho, Krystal Place, Rebecca Salstrand, Monireh Rahmat, Misagh Mansouri, Nancy Fell, Mina Sartipi","doi":"10.1155/2021/5546766","DOIUrl":null,"url":null,"abstract":"<p><p>After short-term, acute-care hospitalization for stroke, patients may be discharged home or other facilities for continued medical or rehabilitative management. The site of postacute care affects overall mortality and functional outcomes. Determining discharge disposition is a complex decision by the healthcare team. Early prediction of discharge destination can optimize poststroke care and improve outcomes. Previous attempts to predict discharge disposition outcome after stroke have limited clinical validations. In this study, readmission status was used as a measure of the clinical significance and effectiveness of a discharge disposition prediction. Low readmission rates indicate proper and thorough care with appropriate discharge disposition. We used Medicare beneficiary data taken from a subset of base claims in the years of 2014 and 2015 in our analyses. A predictive tool was created to determine discharge disposition based on risk scores derived from the coefficients of multivariable logistic regression related to an adjusted odds ratio. The top five risk scores were admission from a skilled nursing facility, acute heart attack, intracerebral hemorrhage, admission from \"other\" source, and an age of 75 or older. Validation of the predictive tool was accomplished using the readmission rates. A 75% probability for facility discharge corresponded with a risk score of greater than 9. The prediction was then compared to actual discharge disposition. Each cohort was further analyzed to determine how many readmissions occurred in each group. Of the actual home discharges, 95.7% were predicted to be there. However, only 47.8% of predictions for home discharge were actually discharged home. Predicted discharge to facility had 15.9% match to the actual facility discharge. The scenario of actual discharge home and predicted discharge to facility showed that 186 patients were readmitted. Following the algorithm in this scenario would have recommended continued medical management of these patients, potentially preventing these readmissions.</p>","PeriodicalId":22054,"journal":{"name":"Stroke Research and Treatment","volume":"2021 ","pages":"5546766"},"PeriodicalIF":1.6000,"publicationDate":"2021-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8390171/pdf/","citationCount":"0","resultStr":"{\"title\":\"Developing a Predictive Tool for Hospital Discharge Disposition of Patients Poststroke with 30-Day Readmission Validation.\",\"authors\":\"Jin Cho, Krystal Place, Rebecca Salstrand, Monireh Rahmat, Misagh Mansouri, Nancy Fell, Mina Sartipi\",\"doi\":\"10.1155/2021/5546766\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>After short-term, acute-care hospitalization for stroke, patients may be discharged home or other facilities for continued medical or rehabilitative management. The site of postacute care affects overall mortality and functional outcomes. Determining discharge disposition is a complex decision by the healthcare team. Early prediction of discharge destination can optimize poststroke care and improve outcomes. Previous attempts to predict discharge disposition outcome after stroke have limited clinical validations. In this study, readmission status was used as a measure of the clinical significance and effectiveness of a discharge disposition prediction. Low readmission rates indicate proper and thorough care with appropriate discharge disposition. We used Medicare beneficiary data taken from a subset of base claims in the years of 2014 and 2015 in our analyses. A predictive tool was created to determine discharge disposition based on risk scores derived from the coefficients of multivariable logistic regression related to an adjusted odds ratio. The top five risk scores were admission from a skilled nursing facility, acute heart attack, intracerebral hemorrhage, admission from \\\"other\\\" source, and an age of 75 or older. Validation of the predictive tool was accomplished using the readmission rates. A 75% probability for facility discharge corresponded with a risk score of greater than 9. The prediction was then compared to actual discharge disposition. Each cohort was further analyzed to determine how many readmissions occurred in each group. Of the actual home discharges, 95.7% were predicted to be there. However, only 47.8% of predictions for home discharge were actually discharged home. Predicted discharge to facility had 15.9% match to the actual facility discharge. The scenario of actual discharge home and predicted discharge to facility showed that 186 patients were readmitted. Following the algorithm in this scenario would have recommended continued medical management of these patients, potentially preventing these readmissions.</p>\",\"PeriodicalId\":22054,\"journal\":{\"name\":\"Stroke Research and Treatment\",\"volume\":\"2021 \",\"pages\":\"5546766\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2021-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8390171/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Stroke Research and Treatment\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2021/5546766\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2021/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stroke Research and Treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/5546766","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
Developing a Predictive Tool for Hospital Discharge Disposition of Patients Poststroke with 30-Day Readmission Validation.
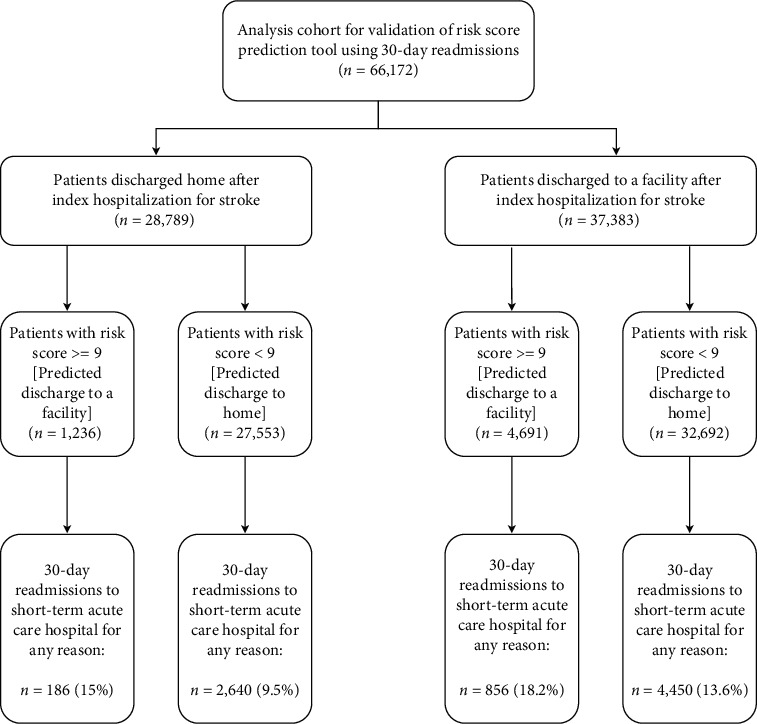
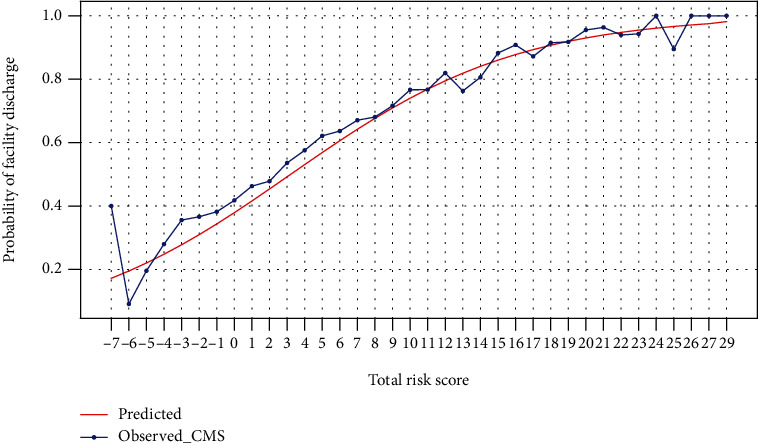
After short-term, acute-care hospitalization for stroke, patients may be discharged home or other facilities for continued medical or rehabilitative management. The site of postacute care affects overall mortality and functional outcomes. Determining discharge disposition is a complex decision by the healthcare team. Early prediction of discharge destination can optimize poststroke care and improve outcomes. Previous attempts to predict discharge disposition outcome after stroke have limited clinical validations. In this study, readmission status was used as a measure of the clinical significance and effectiveness of a discharge disposition prediction. Low readmission rates indicate proper and thorough care with appropriate discharge disposition. We used Medicare beneficiary data taken from a subset of base claims in the years of 2014 and 2015 in our analyses. A predictive tool was created to determine discharge disposition based on risk scores derived from the coefficients of multivariable logistic regression related to an adjusted odds ratio. The top five risk scores were admission from a skilled nursing facility, acute heart attack, intracerebral hemorrhage, admission from "other" source, and an age of 75 or older. Validation of the predictive tool was accomplished using the readmission rates. A 75% probability for facility discharge corresponded with a risk score of greater than 9. The prediction was then compared to actual discharge disposition. Each cohort was further analyzed to determine how many readmissions occurred in each group. Of the actual home discharges, 95.7% were predicted to be there. However, only 47.8% of predictions for home discharge were actually discharged home. Predicted discharge to facility had 15.9% match to the actual facility discharge. The scenario of actual discharge home and predicted discharge to facility showed that 186 patients were readmitted. Following the algorithm in this scenario would have recommended continued medical management of these patients, potentially preventing these readmissions.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
